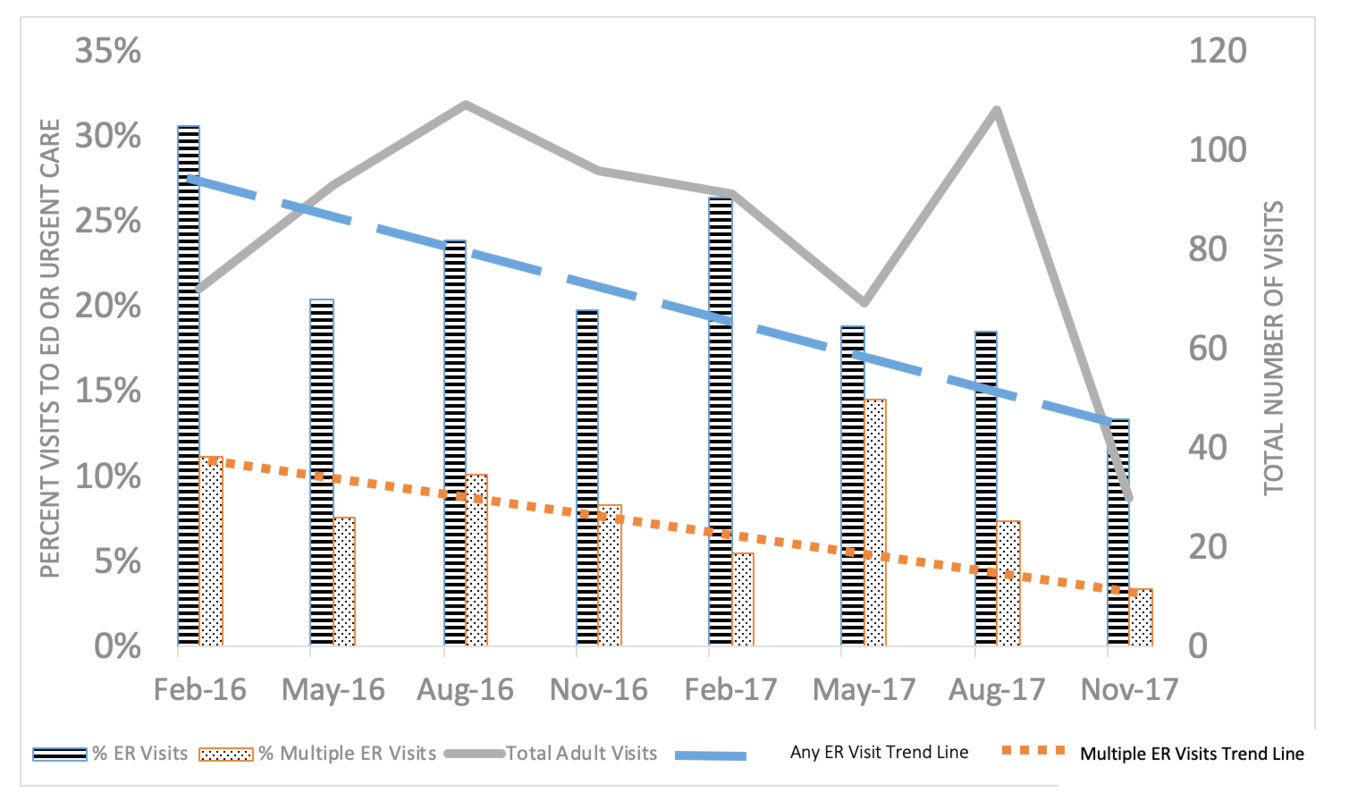
Rationale, aims and objectives. Applying traditional industrial Quality Improvement (QI) methodologies to primary care is often inappropriate because primary care is best thought of as a network of highly interconnected agents in a complex adaptive system (CAS) that is particularly responsive to bottom-up rather than top-down management approaches. We report on a demonstration case study of improvements made in the Family Health Center (FHC) of the JPS Health Network in a refugee patient population that illustrate features of QI in a CAS framework as opposed to a traditional QI approach. Methods. We report on changes in health system utilization by new refugee patients of the FHC from 2016-2017 and summarize relevant theoretical understandings of quality management in complex adaptive systems. Results. Applying CAS principles in the FHC, utilization of the Emergency Department and Urgent Care by newly arrived refugee patients before their first clinic visit was reduced by more than half (total visits decreased from 31% to 14% of the refugee patients). Our review of the literature demonstrates that traditional top-down QI processes are most often unsuccessful in improving even a few single-disease metrics, and increases clinician burnout and penalizes clinicians who care for vulnerable patients. Improvement in a CAS occurs when front-line clinicians identify care gaps and are given the flexibility to learn and self-organize to enable new care processes to emerge, which are created from bottom-up leadership that utilize existing interdependencies made more sustainable as front-line clinicians use sensemaking to improve care processes. Conclusions and future directions. Recent reforms announced in primary care in Scotland, a few examples in the medical literature, and statements from some healthcare system leaders are examples of early adapters who are applying the principles of CAS to their QI efforts. Such initiatives and our example provide models for others to follow.