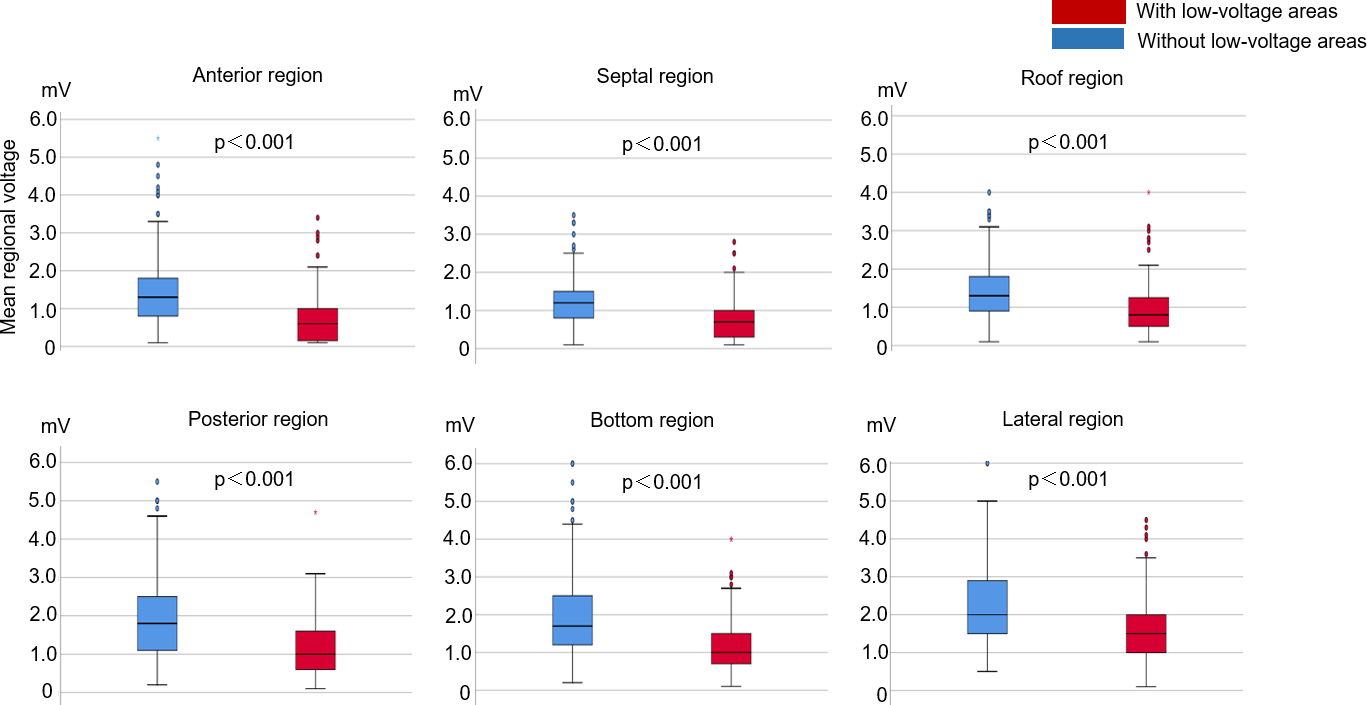
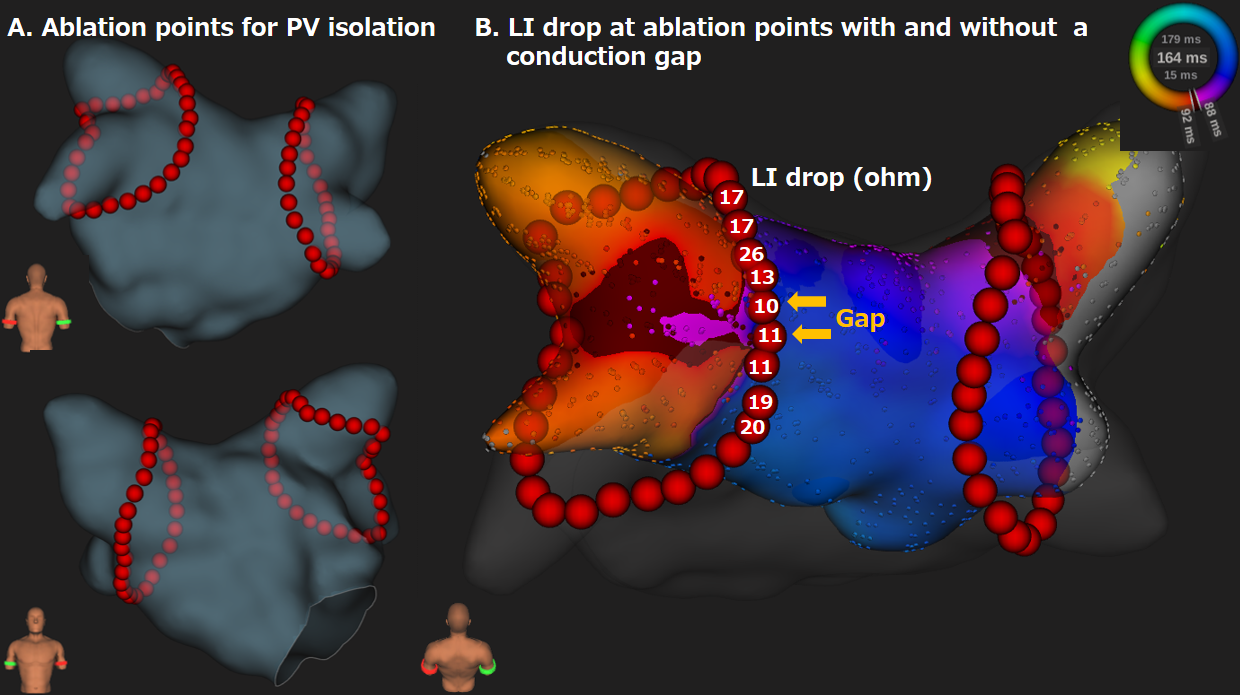
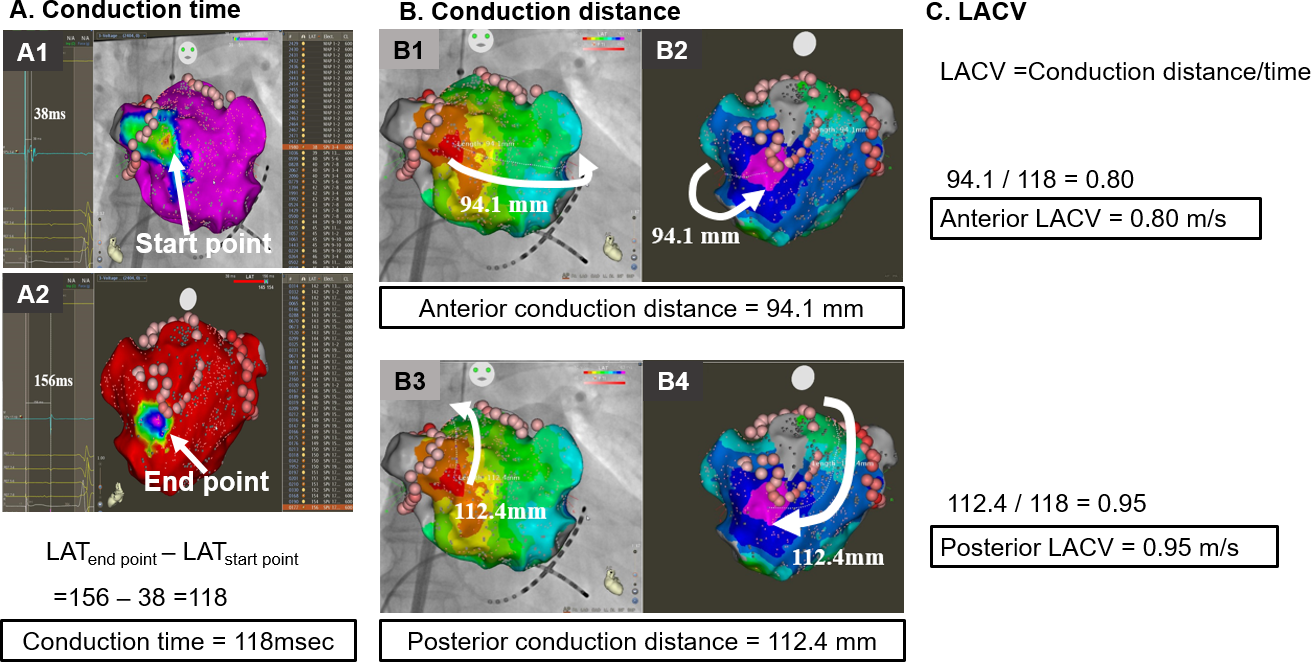
Background: Atrial conduction velocity may represent atrial fibrillation (AF) substrate after pulmonary vein isolation (PVI). To elucidate the association between whole left atrial conduction velocity (LACV) and AF recurrence after PVI. Methods and Results: This observational study enrolled 279 patients who underwent PVI alone as an initial AF ablation procedure. After PVI, the left atrium was mapped with a 20-pole multielectrode in conjunction with the CARTO3 system during 100-ppm right atrial pacing. Left atrial conduction distance and conduction time were calculated from the start to the end of the propagation wave front in the left atrium. LACVs on the anterior and posterior routes were calculated as conduction distance divided by conduction time. Anterior and posterior LACVs were slower in patients with AF recurrence than in those without (anterior, 0.79 [0.71, 0.86] vs. 0.96 [0.90, 1.06], p < 0.001; posterior, 0.99 [0.89, 1.14] vs. 1.10 [1.00, 1.29], p < 0.001). AF recurrence was best predicted by anterior LACV with a cut-off value of 0.87 m/s (sensitivity 87%, specificity 81%, and predictive accuracy 84%). Multivariate analysis demonstrated that a slow anterior LACV < 0.87 m/s was an independent predictor of AF recurrence with an adjusted hazard ratio of 11.8 (6.36 – 22.0). Patients with anterior low-voltage areas demonstrated slower anterior LACV than those without low-voltage areas (0.89 [0.71, 1.00] vs. 0.94 [0.87, 1.05], p < 0.001). Conclusion: A slow LACV in the entire left atrium was an excellent predictor of AF recurrence after PVI, suggesting the necessity of additional ablations.