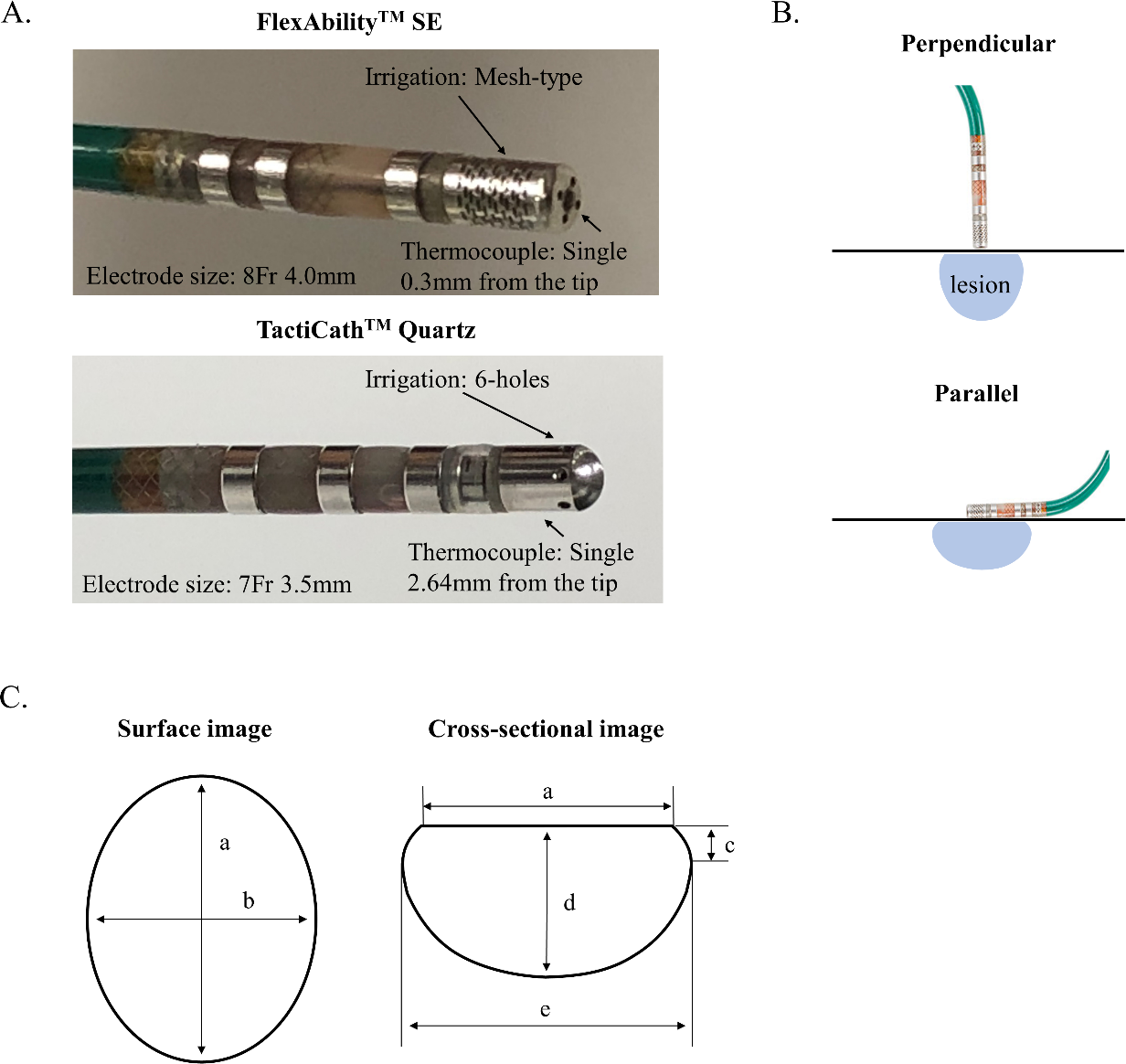
Background & Objectives The FlexAbilityTM SE catheter has a laser-cut 8Fr 4-mm flexible tip irrigated through laser-cut kerfs with a thermocouple 0.3mm from the distal end. The TactiCathTM SE catheter has an 8Fr 3.5-mm tip and 6-irrigation port with a thermocouple 2.67mm proximal to the tip. We investigated the impact of these differences on the efficacy and safety of RF-applications. Methods RF applications at a range of powers (20W, 30W, and 40W), contact forces (5g, 15g, and 25g), and durations (10-60s) using perpendicular/parallel catheter orientation, were performed in excised porcine hearts. Lesion characteristics and incidence of steam pops were compared. Results 540 lesions were examined. The FlexAbilityTM SE catheter produced smaller lesion depths (4.0mm vs. 4.4mm, p=0.014 at 20W; 4.6mm vs. 5.6mm, p=0.015 at 30W), surface areas (22.7mm2 vs. 29.2mm2 at 20W, p=0.005; 23.2mm2 vs. 28.7mm2, p=0.009 at 30W) and volumes (126.1mm3 vs. 175.1mm3, p=0.018 at 20W; 183.2mm3 vs. 304.3mm3, p=0.002 at 30W) with perpendicular catheter placement. However, no differences were observed with parallel catheter placement. Steam-pops were significantly less frequently observed with the FlexAbilityTM SE catheter (4% vs. 22%, p<0.001) irrespective of catheter direction to the tissue. Multivariate analysis showed that use of the TactiCathTM SE catheter, power ≥40W, contact force ≥25g, RF duration >30s, parallel angle and impedance drop ≥20Ω were significantly associated with occurrence of steam-pops. Conclusions The FlexAbilityTM SE catheter reduced the risk of steam-pops, but produced smaller lesions with perpendicular catheter placement compared to the TactiCathTM SE catheter.