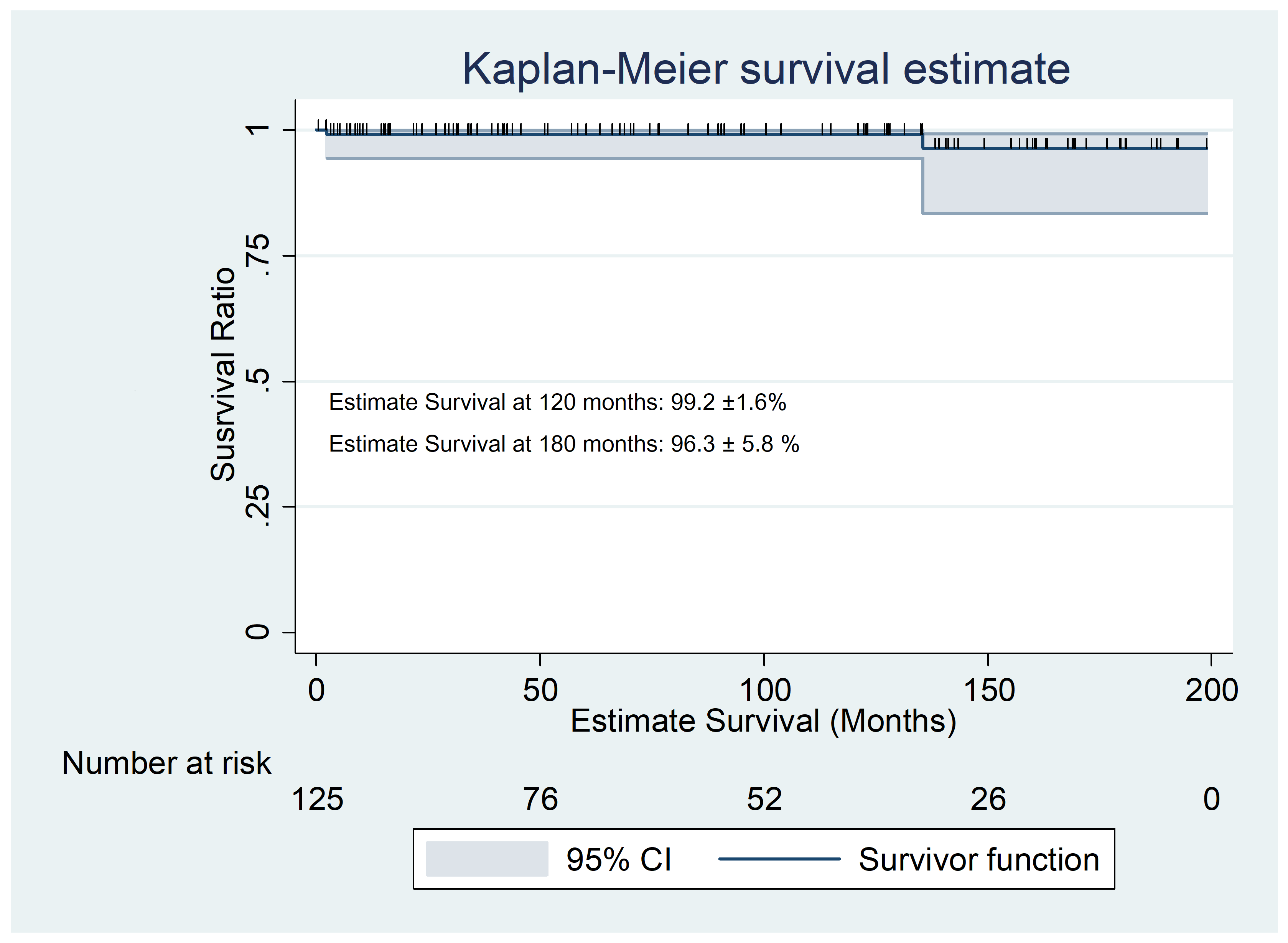
Background and Aim of the Study: Barlow’s disease is characterized by excess myxomatous degenerative tissue, leaflets prolapse and/or billowing, chordal-elongation, and annular-dilation. We reviewed our experience in Minimally Invasive Mitral Valve Repair (MIMVR) techniques to treat this complex mitral pathology. Methods: Between 1999 and 2017 a group of 125 patients was identified as Barlow’s disease undergoing MIMVR. The diagnosis of Barlow disease was based upon preoperative transesophageal-echocardiography (TEE) and confirmed by the surgeon’s assessment during open-heart procedure. Operative technique and data were retrospectively collected along with intra-hospital and long-term follow-up. Results: Successful Mitral Repair was possible in 100% of cases (125 patents) within the first cross clamp. Most patients (118 – 94.4%) were treated by the Edge to Edge (Alfieri-Stich), while 2 (1.6%) where corrected by neochordae implant and 2 (1.6%) by quadrangular resection. 58 patients (47.1%) received complete semi-rigid ring, while 65 (52.9%) incomplete flexible partial ring excluding the LAM. Concomitant procedures were additional cleft occlusion in 10 cases (8%), tricuspid valve repair (ring implant or remodeling) in 29 cases (23.2%), left atrial ablation for atrial fibrillation in 4 cases (3.2%) and atrial septal repair in 4 (3.2%). Operative mortality was 0%. Average long-term follow-up was 85 ± 62 months, with a survival rate of 97.6%, freedom from redo mitral surgery of 98.4% and freedom from >2+ recurrent mitral regurgitation of 94.5%. No difference in outcome could be related to annuloplasty ring type. Conclusions: Mitral repair can be safely and successfully achieved though minimal-invasive approach, with optimal long-term results.