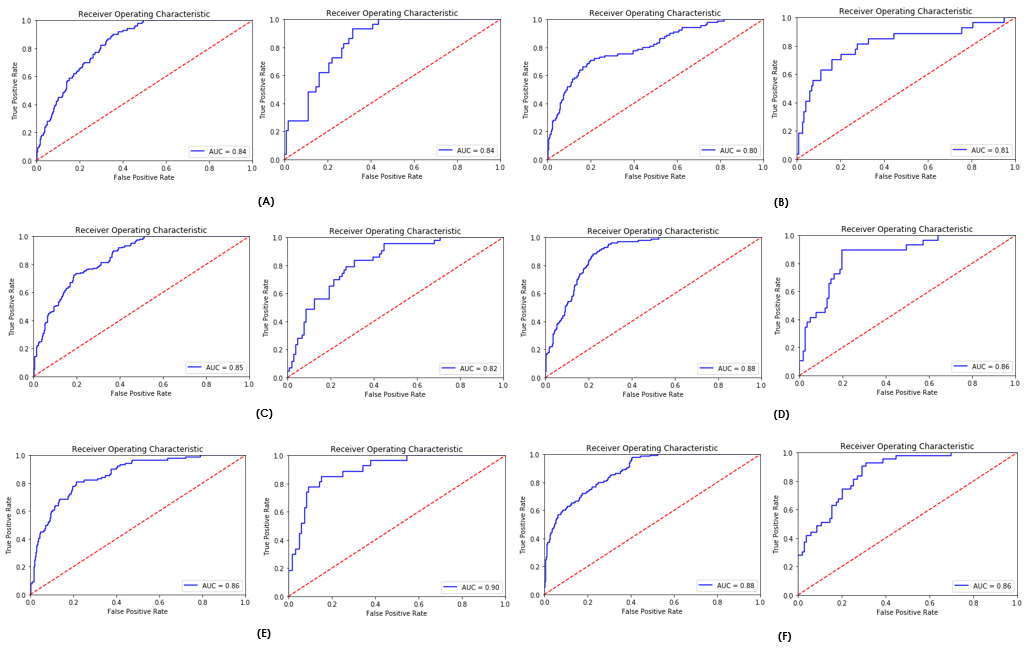
Objective: To establish a prediction model of clinical outcomes in women with placenta accreta spectrum (PAS) Design: Retrospective cohort study Setting: International multicenter study (PAS-ID); 11 centers from 9 countries Population: Women who were diagnosed with PAS and were managed in recruiting centers between January 1st, 2010 and December 31st, 2019. Methods: Data were collected using a standardized sheet, which included baseline information, medical and obstetric history, diagnosis, disease characteristics, management, and outcomes. Analysis of association between these variables and primary outcome was first conducted using conventional logistic regression. Data were reanalyzed using machine learning (ML) models, and 2 models were created to predict outcomes using antepartum and perioperative features. Main Outcome Measures: Massive PAS-associated perioperative blood loss (intraoperative blood loss ≥ 2500 ml, triggering massive transfusion protocol, or complicated by disseminated intravascular coagulopathy). Other outcomes include prolonged hospitalization > 7 days and admission to intensive care unit (ICU). Results: 727 women with PAS were included. Area under curve (AUC) for ML antepartum prediction model was 0.84, 0.81, and 0.82 for massive blood loss, prolonged hospitalization, and admission to ICU, respectively. Significant contributors to this model were parity, placental site, method of diagnosis and antepartum hemoglobin. Combing baseline and perioperative variables, ML model performed at 0.86, 0.90, and 0.86 for study outcomes, respectively. This model was most contributed by ethnicity, pelvic invasion, and uterine incision. Conclusions: ML models may be used to calculate individualized risk of morbidity in women with PAS, which may assist to outline management plan in priori