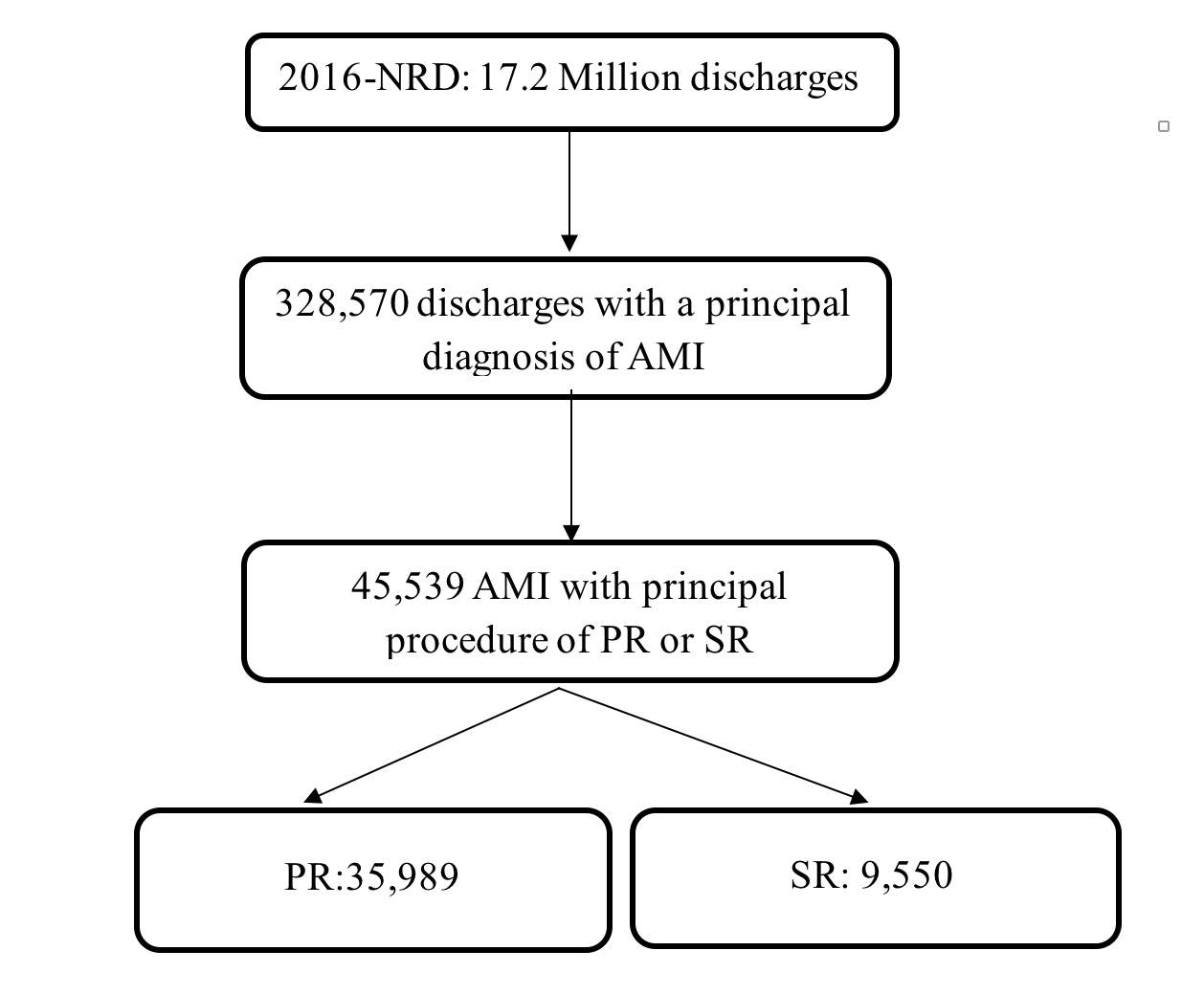
Acute myocardial infarction (AMI) is a common medical condition that requires appropriate revascularization in a timely manner. Percutaneous revascularization (PR) was the first line treatment option when feasible. Limited data is available comparing PR to surgical revascularization (SR) in the AMI setting. Study population was extracted from the 2016 Nationwide Readmissions Data using International Classification of Diseases, tenth edition codes for AMI, PR, SR, and procedural complications. Endpoints included in-hospital all-cause mortality, length of index hospital stay (LOS), stroke, acute kidney injury, bleeding, blood transfusion, acute respiratory failure, and total hospital charges. The study identified 45,539 discharges with a principal admission diagnosis of AMI who had either PR or SR as a principal procedure. Single vessel revascularization was performed in 67.8% (93.1% had PR versus 6.9% had SR, p<0.01). Multivessel revascularization was performed in 32.2% (64.8% had PR versus 35.2% had SR, p<0.01). In comparison to SR, PR was associated with higher in-hospital all-cause mortality (P<0.01), shorter LOS (p<0.01), and lower incidence of post-procedural stroke (p<0.01), acute kidney injury (p<0.01), bleeding (p<0.01), need for blood transfusion (p<0.01), acute respiratory failure (p<0.01), and total hospital charges (p<0.01). In a subgroup analysis, SR mortality benefit persisted in patients who had multivessel revascularization, but not in single vessel revascularization. In patients presented with AMI, PR was associated with higher in-hospital all-cause mortality but lower morbidity, shorter LOS, and lower total hospital charges than SR. However, the mortality benefit of SR was seen in multivessel revascularization only, and not in single vessel revascularization.