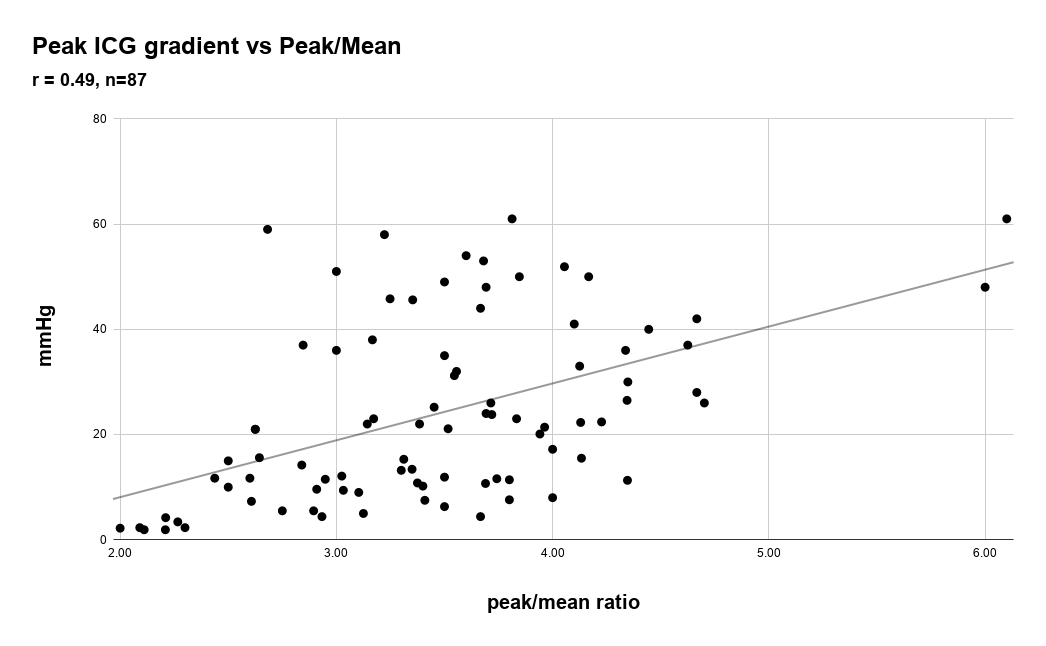
Controversy surrounds the cause of the pressure gradient in patients with hypertrophic obstructive cardiomyopathy (HOCM). Left ventricular cavity obliteration (LVCO) was first described as the cause of the gradient but subsequently systolic anterior motion (SAM) of the mitral valve has been established as the cause. Nevertheless, the two gradients, though different in origin and significance, share similar characteristics. They both have a similar “dagger” profile, are obtained from the cardiac apex, are associated with a hyperdynamic left ventricle, and the gradients are worsened by Valsalva. The distinction has clinical relevance, because treating the intra cavitary gradient (ICG) of LVCO as if it were a SAM associated gradient associated with HOCM would be inappropriate and possibly harmful. To clarify the cause and characteristics of the ICG in patients with LVCO in patients without HOCM we assessed the extent and duration of cavity obliteration and for differentiation we compared the spectral profiles with patients with HOCM and severe aortic stenosis (AS). Higher ICG is associated with greater extent and more prolonged apposition of LV walls. The spectral profile of patients with AS, HOCM and LVCO are differentiated by the peak/mean gradient ratios of 2 or less, 2-3, and 3 or greater, respectively in > 90% of patients. Most patients with LVCO without HOCM or severe LVH have an ICG < 36 mmHg. The magnitude of ICG is quantitatively associated with extent and duration of LVCO. Spectral profiles of severe AS, HOCM, and LVCO can be differentiated by the peak/mean gradient ratio.