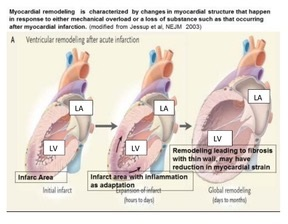
Chronic heart failure (CHF) has different stages and they include pre-HF (PHF), a state of high risk of developing myocardial dysfunction and subsequently, advanced CHF (ACHF). Some major behavioral risk factors of PHF are Western diet, tobacco, alcoholism, sedentary life style and chronic mental disorders (anxiety, depression). These insults might predispose to biological risk factors such as obesity, diabetes mellitus dyslipidemia hypertension, myocardial infarction and cardiomyopathy. These risk factors damage the myocytes leading to fibrosis, apoptosis, cardiac hypertrophy, along with alterations in cardiomyocyte’ size and shape. A condition of physiological subcellular remodeling resulting into a pathological or deformation state might be developed conductiong to PHF. Both PHF and HF are associated with the activation of phospholipases and protease, mitochondrial dysfunction, oxidative stress and development of intracellular free Ca2+ [Ca2+]i overloading or an elevation in diastolic [Ca2+]i. Simultaneously, cardiac gene expression is activated leading to further molecular, structural and biochemical changes of the myocardium. The sub-cellular remodeling may be intimately involved in the transition of cardiac hypertrophy to heart failure. Two-dimensional (2D) and three-dimensional (3D) speckle tracking-echocardiography (STE) have been used to quantify regional alterations of longitudinal strain and area strain, through their polar projection, which permits a further assessment of both sites and degrees of myocardial damage. The examination of strain can identify sub-clinical cardiac dysfunction or cardiomyocyte remodeling. It is concluded that during remodeling of the myocardium, cardiac strain is attenuated which can be used for the assessment of disease progression and subsequently for therapeutic interventions.