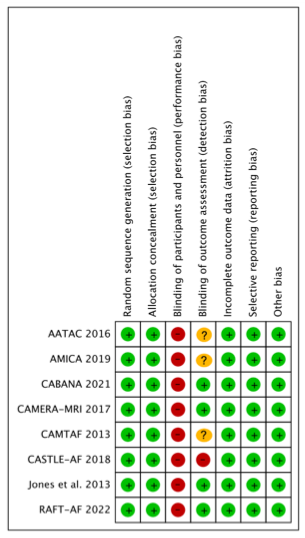
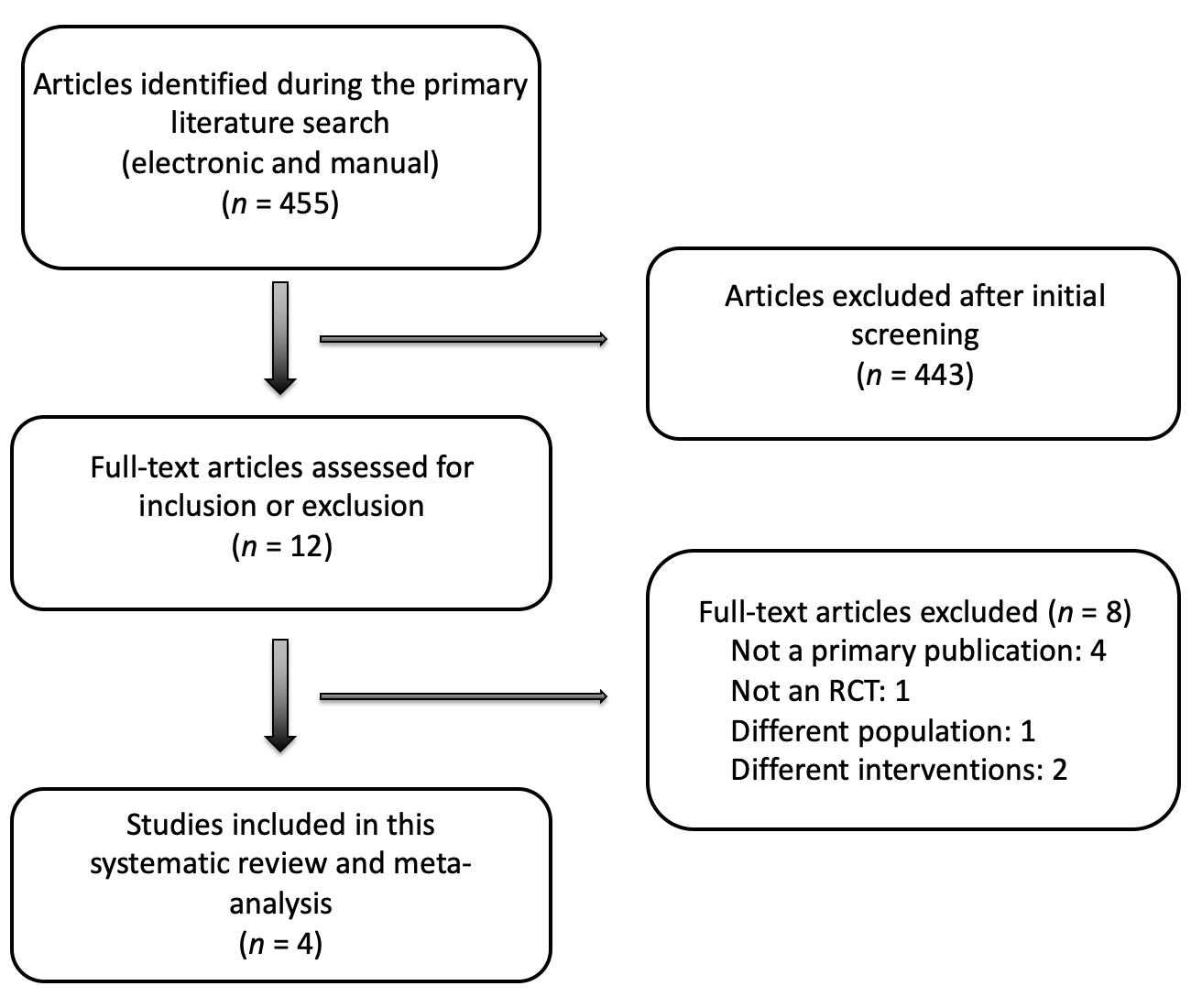
Introduction: Increasing evidence has suggested improved outcomes in atrial fibrillation (AF) patients with heart failure (HF) undergoing catheter ablation (CA) as compared to medical therapy. We sought to investigate the benefit of CA on outcomes of patients with AF and HF as compared to medical therapy. Methods and Results: A systematic review of PubMed, Embase, and Cochrane Central Register of Clinical Trials was performed for clinical studies evaluating the benefit of CA for patients with AF and HF. Primary endpoint was all-cause mortality. Secondary endpoints included atrial-arrhythmia recurrence and improvement in left ventricular ejection fraction (LVEF). Eight randomized controlled trials were included with a total of 2121 patients (mean age: 65 ± 5 years; 72% male). Mean follow-up duration was 32.9 ± 14.5 months. All-cause mortality in patients who underwent CA was significantly lower than in the medical treatment group (8.8% vs. 13.5%, RR 0.65, 95% CI 0.51-0.83, P=0.0005). A 35% relative risk reduction and 4.7% absolute risk reduction in all-cause mortality was observed with CA. Rates of atrial-arrhythmia recurrence were significantly lower in the CA group (39.9% vs 69.6%, RR 0.55, 95% CI 0.40-0.76, P=0.0003). Improvement in LVEF was significantly higher in patients undergoing CA (+9.4 ±7.6%) as compared to conventional treatment (+3.3±8%) (Mean difference 6.2, 95% CI 3.6-8.8, P<0.00001). Conclusion: CA for AF in patients with HF decreases all-cause mortality, improves atrial-arrhythmia recurrence rate and LVEF when compared to medical management. CA should be considered the treatment of choice to improve survival in this select group of patients.