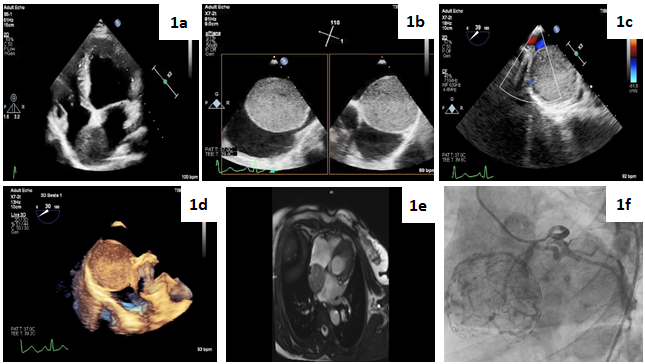
A previously healthy 68-year-old woman presented to the outpatient clinic with a 2-month history of palpitation. Physical examination and laboratory findings were unremarkable. Her electrocardiogram showed sinus tachycardia with a heart rate of 115 beats/m. Transthoracic echocardiography (TTE) showed a normal ejection fraction with a huge mass in the left atrium (Figure 1a). Transesophageal echocardiography (TEE) and cardiac magnetic resonance imaging (MRI) were performed for further evaluation. TEE revealed a hyperechogenic, well-demarcated mass in the left atrium, that was attached to the interatrial septum and adjacent to the left pulmonary veins (Figure 1b, 1c,1d). Cardiac MRI revealed a heterogeneous left atrial mass located on the fossa ovalis, 58x52x54 mm in size and markedly hyperintense on a STIR sequence (Figure 1e). These findings were suggestive of a benign cardiac tumour such as myxoma or hemangioma. A decision for surgery was made and coronary angiography was performed which showed that the branch of the circumflex artery supplied and surrounded the mass in the form of a net (Figure 1e). The patient underwent complete excision of the mass (Figure 2a, 2b). Histopathological examination revealed a nested architecture of epitelioid cells, the nests are round or oval in shape and invested by an fibrovascular stroma. Tumor cells had centrally and eccentrically located round nuclei and cytoplasm ranging from finely granular to eosiniphilic. At immunohistochemical staining, the nests were positive for chromogranin A, negative for cytokeratin (Figure 2c, 2d, 2e, 2f). A diagnosis of paraganglioma was made. After an uneventful postoperative course, she was discharged home on postoperative day 6. Cardiac paraganglioma is a very rare neuroendocrine tumour and accounts for less than 1% of primary cardiac tumours (1,2). Approximately 10% of paragangliomas may be malignant, complete surgical resection remains the first-line treatment (3).