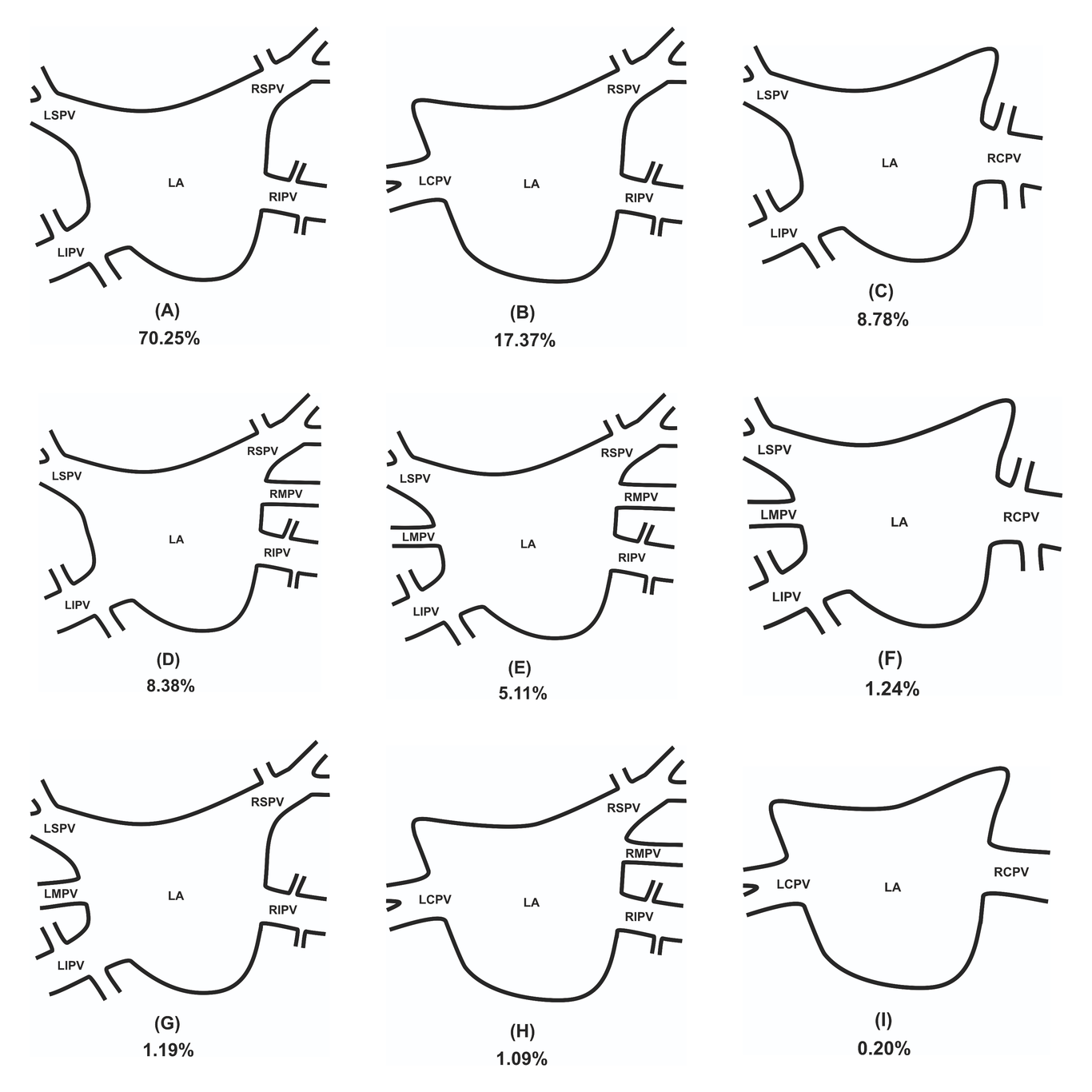
Introduction: The aim of this study was to establish the most accurate and up-to-date anatomical knowledge of PVs ostia variations, diameters and ostial area, in order to provide physicians, especially heart and thoracic surgeons with exact knowledge concerning this area. Materials and methods: Major online medical databases such as PubMed, Embase, Scopus, Web of Science and Google Scholar were searched to gather all studies in which the variations, maximal diameter and ostial area of the PVs were investigated. During the study, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed. Additionally, The Critical Appraisal Tool for Anatomical Meta-analysis (CATAM) was used to provide the highest quality findings. Reults: The most common ostia variation is classical one, containing left superior pulmonary vein (LSPV), left inferior pulmonary vein (LIPV), right superior pulmonary vein (RSPV) and right inferior pulmonary vein (RIPV). Mean diameters and ostial areas of each pulmonary vein were established in general population and in multiple variations considering method of gathering the data and geographical location. Conclusion: Significant variability in PV ostia is observed. Left-sided PVs have smaller ostia than corresponding right-sided PVs, and the inferior PVs ostia are smaller than superior. The size of the LCPV ostium is the largest among all analyzed veins, while the ostium of RMPV is the smallest. It is hoped that the results from this meta-analysis will help clinicians in planning and performing procedures that involve pulmonary and cardiac area.