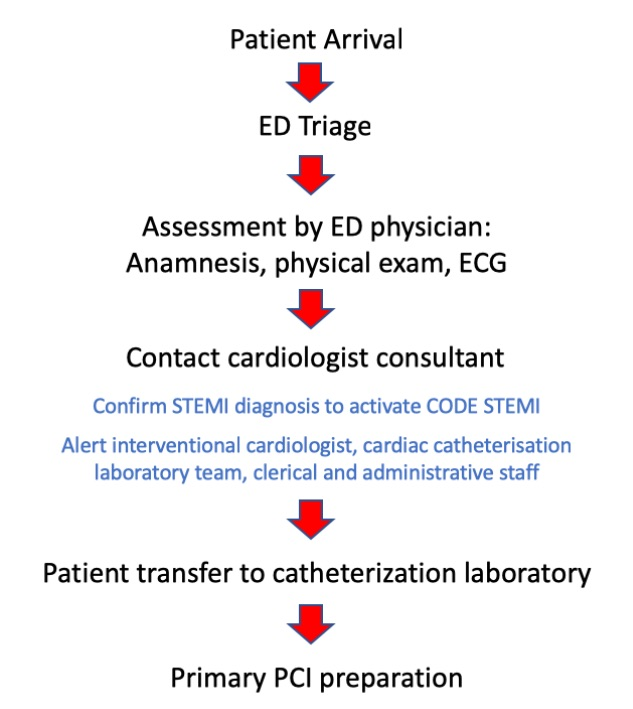
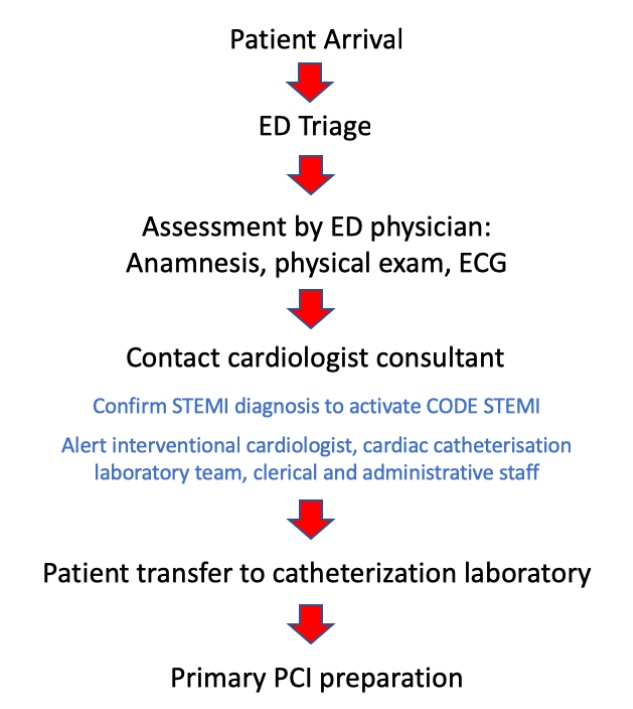
Background : One of the highest causes of cardiac mortality is ST Elevation Myocardial Infarction (STEMI). Delay in the management of STEMI patients resulted high mortality, morbidity, and economic burden. CODE STEMI is a protocol to reduce door to balloon time and improve patient’s quality care and clinical outcome. Objectives : To determine the effect of the implementation of CODE STEMI on clinical outcome and cost efficiency of a quality care of STEMI patients at Dr. Cipto Mangunkusumo General Hospital. Method: This is a retrospective cohort study that reviewed 207 medical records of STEMI patients who underwent primary percutaneous coronary intervention (PPCI) in 2015-2018. The patients were divided into two groups. The first group was treated prior to establishing the CODE STEMI and the other group was treated with CODE STEMI protocol. The primary outcome was to measure in-hospital mortality and morbidity and total hospital cost between both groups. Secondary end-points included length of stay (LOS) and Cost Efficient Analysis. Data analysis was done using Mann Whitney and Chi square test. Results: There were 72 and 135 patients in Pre‐CODE STEMI and CODE STEMI groups respectively. In CODE STEMI group, median D2BT was significantly reduced by 130 min (P< 0.001), median LOS was reduced by 1 day (P=0.009) and there was cost reduction by approximately USD 1,000. There were declining trend of in-hospital mortality rates (8.3% vs 4.4%) and MACE at 30 days (48.61% vs 37.78%). Conclusion: Implementation of CODE STEMI can improve clinical outcome, reduce length of stay and cost efficiency of STEMI patients in general hospitals.