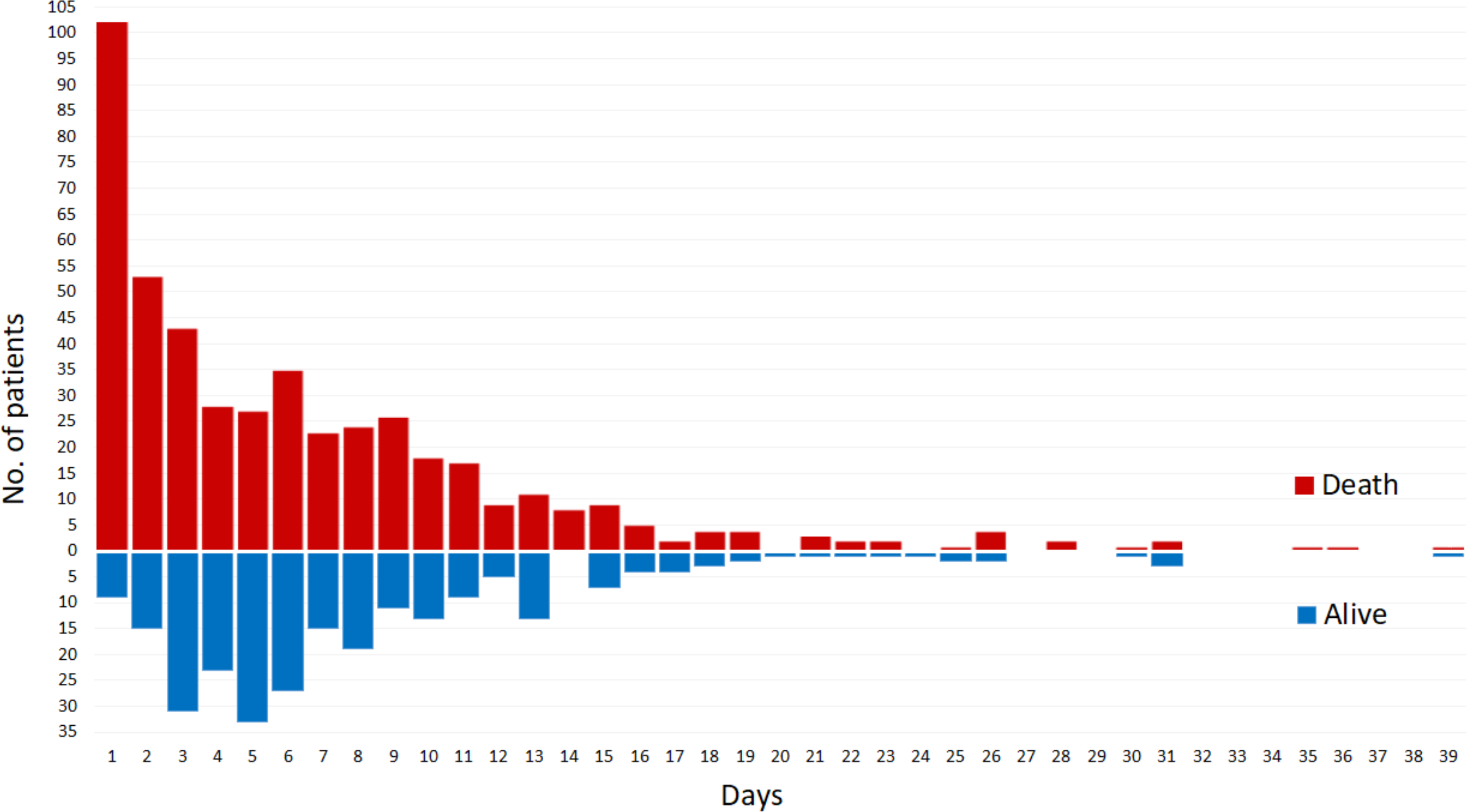
Background and Aim: The optimal duration of veno-arterial extracorporeal membrane oxygenation (VA-ECMO) in patients affected by postcardiotomy cardiogenic shock (PCS) remains controversial. We aimed to investigate the impact of VA-ECMO duration on hospital outcomes. Methods: Data on PCS patients receiving VA-ECMO were retrieved from the multicentre PC-ECMO registry. Patients were stratified according to different duration of VA-ECMO therapy: ≤3 days, 4-7 days, 8-10 days, and >10 days. Results: A total of 725 patients with a mean age of 62.9±12.9 years were included. The mean duration of VA-ECMO was 7.1±6.3 days (range: 0-39 days), and 39.4% patients were supported for ≤3 days, 29.1% for 4-7 days, 15.3% for 8-10 days, and finally 20.7% for >10 days. A total of 391 (53.9%) patients were successfully weaned from VA-ECMO while 134 (34.3%) died prior to discharge. Multivariable logistic regression showed that prolonged duration of VA-ECMO therapy (4-7 days, adjusted rate 53.6%, odds ratio [OR] 0.28, 95% confidence interval [CI] 0.18-0.44; 8-10 days, adjusted rate 61.3%,OR 0.51, 95% CI 0.29-0.87; and >10 days, adjusted rate 59.3%,OR 0.49, 95% CI 0.31-0.81) was associated with lower risk of mortality compared with VA-ECMO lasting ≤3 days (adjusted rate 78.3%). Patients requiring VA-ECMO therapy for 8-10 days (OR 1.96, 95% CI 1.15-3.33) and >10 days (OR 1.85, 95% CI 1.14-3.02) had significantly higher mortality compared to those on VA-ECMO for 4-7 days. Conclusions: PCS patients weaned from VA-ECMO after 4 to 7 days of support had significantly lower mortality compared with those with shorter or longer mechanical support.