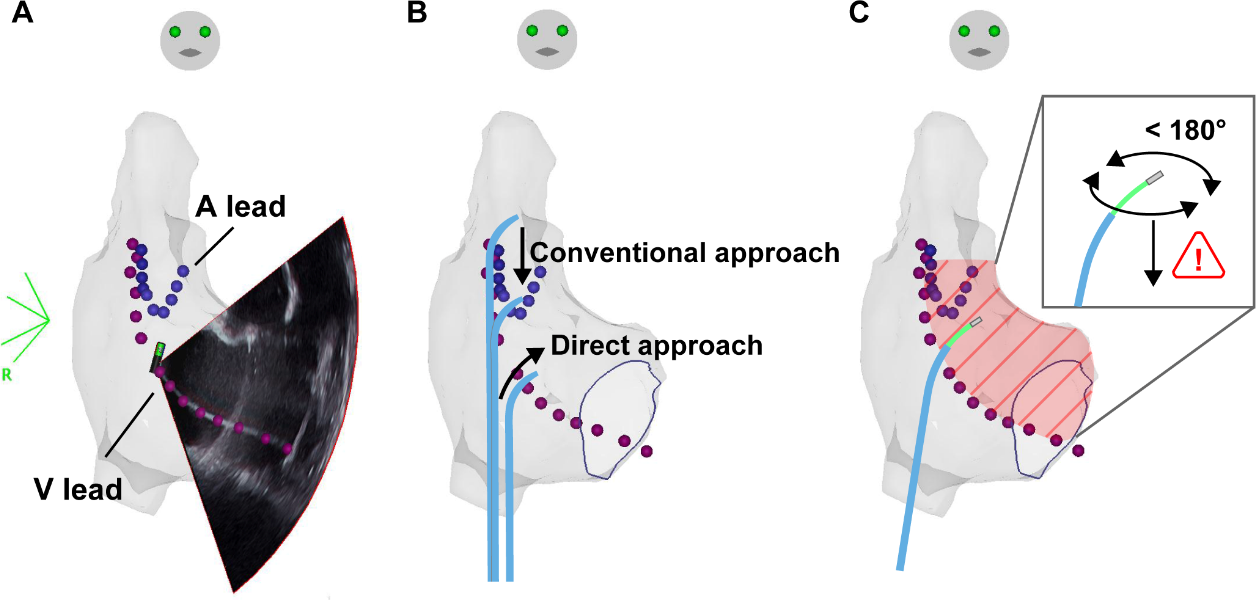
Introduction: Utilizing a 3-dimensional (3-D) mapping system and intracardiac echocardiography (ICE) has allowed ablation procedures with less or without fluoroscopy; however, there is limited data for patients with cardiac electronic implantable device (CIED) leads regarding the suspected risk of lead injury. Therefore, we sought to explore technics to perform safe trans-septal approach and catheter manipulation technique in patients with CIED leads. Methods and Results: This study comprised 68 consecutive patients (45 [66.2%] males, median [interquartile range] 73 [68–77] years old) with CIED who underwent catheter ablation for supraventricular tachycardia, 16 without fluoroscopy (zero-fluoro group) and 52 with fluoroscopy (conventional-fluoro group), between July 2019 and April 2021. All procedures were performed under a 3-D mapping system and ICE guidance. We compared the differences in treatment and development of complications between the two groups. The procedures were mainly atrial fibrillation (73.6%) and atrial tachycardia. The median time from venipuncture to trans-septal procedure (zero-fluoro vs. conventional-fluoro group: 27.0 min vs. 23.5 min, P=0.71) and total procedure time (215 min vs. 172 min, P=0.55) were not different between the two groups. The acute procedural success rate (100% vs. 98.1%, P=1.00) and reduction of atrial high-rate episodes at 6 months (3.2 [0.3–93.9]% vs. 1.0 [0.0–14.9]%, P=0.33) did not differ between the two groups. No patient showed lead-related complications in both groups. Conclusions: Zero-fluoro ablation for supraventricular arrhythmia using 3-D mapping and ICE in patients with CIED leads was feasible under careful catheter manipulation.