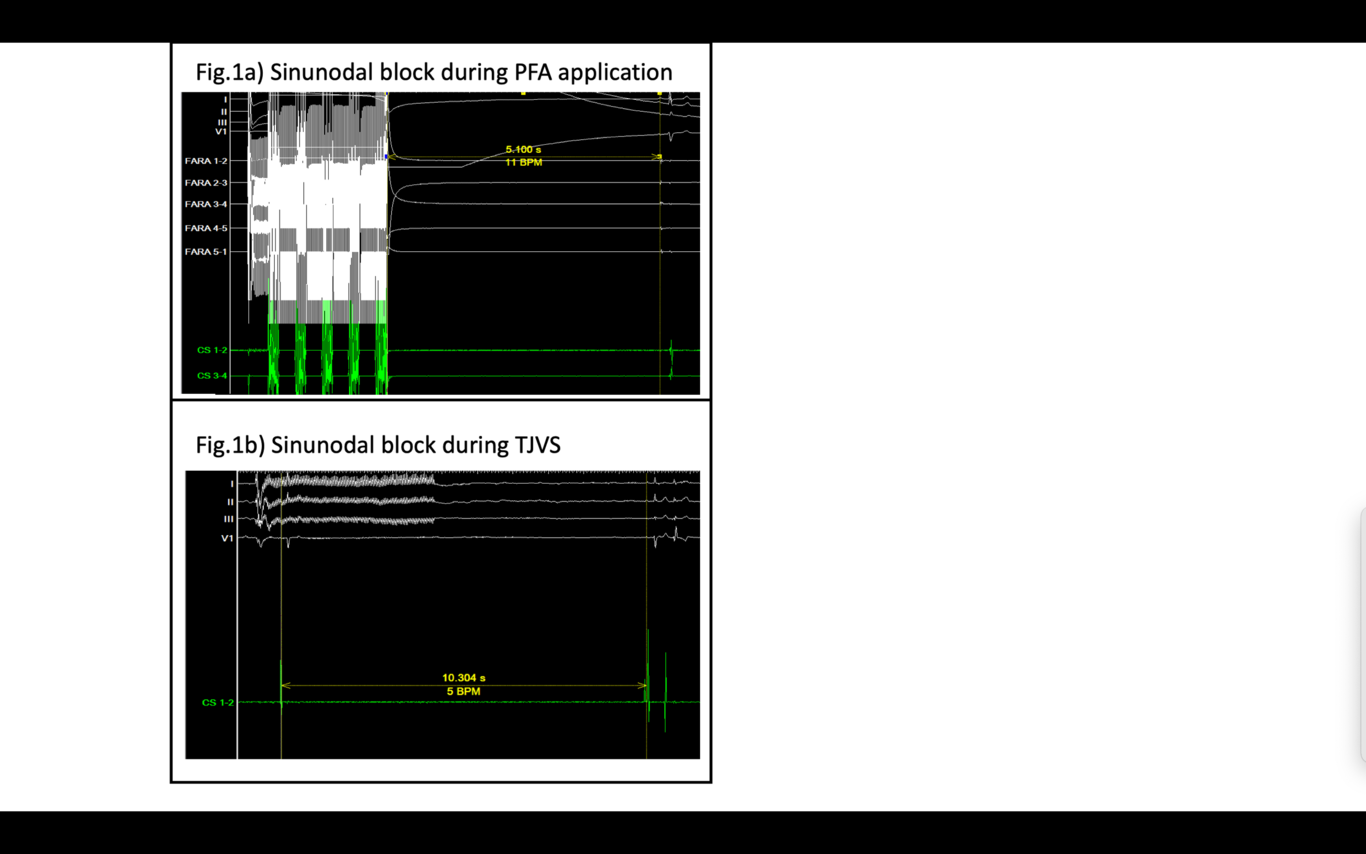
Background: Pulsed field ablation (PFA) is a novel technique for pulmonary vein isolation in atrial fibrillation management. Notably, asystole episodes of varying durations have been observed during electroporation, but the underlying mechanisms remain unclear. Objective: This study hypothesizes that asystole during PFA is attributable to the activation of parasympathetic ganglia on the left atrium’s surface. Methods: We conducted a study with 24 patients (67% male, 62.8 ± 11.0 years, BMI: 25.3 ± 5.6) suffering from paroxysmal atrial fibrillation. The order of pulmonary veins chosen for electroporation was randomized to avoid cumulative electroporation effects. PFA was performed and the duration of cardiac pauses post-electroporation was recorded for each application. To examine the impact of electroporation on the parasympathetic nervous system, transjugular vagal stimulation (TJVS) was performed from the right internal jugular before and after isolation of each vein, during sinus rhythm and atrial pacing. Continuous data were analyzed with Student’s t-tests or Mann-Whitney U tests as appropriate; nominal data were evaluated using chi-square or Fisher exact tests. Results: Pre-PFA TJVS induced sinus pauses of 10.1 ± 2.74 seconds. A sinus block of over 3 seconds was present in 23 out of 24 patients. Post-PFA, the Right Superior Pulmonary Vein (RSPV) showed the highest decrease of TJVS-induced sinus pauses (RSPV: before 8.41 ± 4.53 vs after 3.27 ± 3.53 sec, p<0.001, RIPV: before 6.76 ± 4.54 sec vs. 6.89 ± 5.07 sec, p=0.90; LSPV: before 6.76 ± 5.25 sec vs. after 6.93 ± 4.29 sec, p=0.61; LIPV: before 7.80 ± 4.06 sec vs. after 7.88 ± 3.84 sec, p=0.91). Notably, sinus blocks over 3 seconds decreased significantly after RSPV ablation (19 before PFA, 10 after PFA, p<0.01), with less dramatic changes in other veins (RIPV: before 19, after 16, p=0.33; LSPV: before 14, after 19, p=0.11; LIPV: before 21, after 21, p=1.00). RSPV PFA also had the strongest impact on TJVS-induced AV block duration compared to the remaining veins (RSPV: before 6.49 ± 3.48 vs after 4.07 ± 3.27 sec, p<0.01, RIPV: before 6.00 ± 3.29 sec vs. 4.58 ± 3.99 sec, p=0.08; LSPV: before 5.15 ± 3.94 sec vs. after 5.14 ± 3.48 sec, p=0.93; LIPV: before 6.06 ± 3.98 sec vs. after 5.83 ± 3.44 sec, p=0.38). The incidence of AV blocks over 3 seconds was markedly reduced post-RSPV and post RIPV ablation (RSPV: before:19 vs. after: 14, p=0.11, RIPV: before:19 vs. after: 14, p=0.11), with minor changes in other veins (LSPV: before 14, after 16, p=0.55; LIPV: before 17, after 18, p=0.77). Conclusions: PFA applications during pulmonary vein isolation have acute effect on the autonomic nervous system, as evidenced by the decrease in TJVS-induced sinus and atrioventricular block at the level of the right superior pulmonary vein. PFA-induced pauses are more frequent during applications on the LSPV, and less frequent when prior isolation of the RSPV has been performed, suggesting a vagally-mediated mechanism involving the right superior and/or right posterior ganglionated plexi.