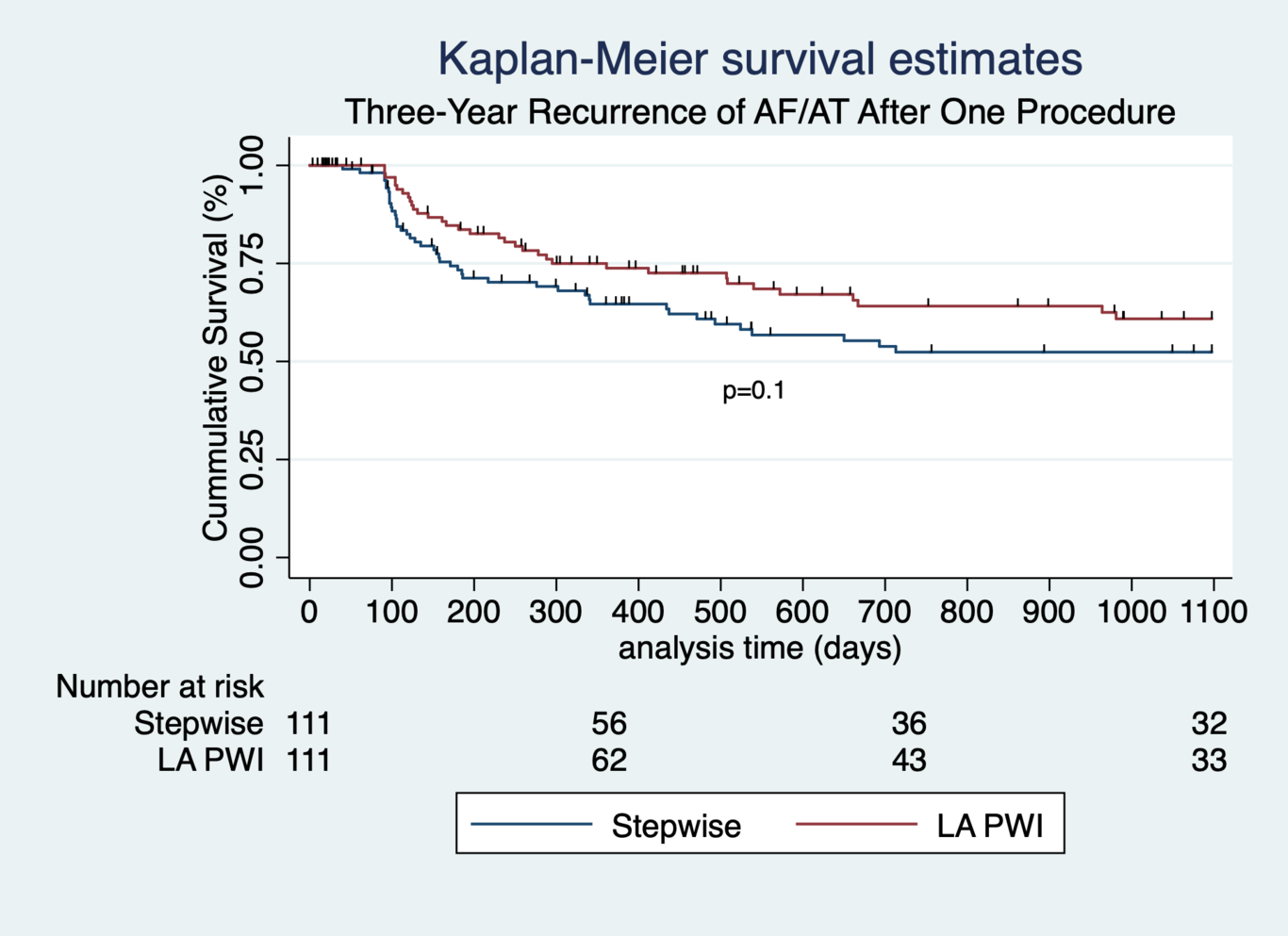
Objective: To compare multiple-procedure catheter ablation outcomes of a stepwise approach versus left atrial posterior wall isolation (LA PWI) in patients undergoing non-paroxysmal atrial fibrillation (NPAF) ablation. Background: Unfavorable outcomes for stepwise ablation of NPAF in large clinical trials may be attributable to pro-arrhythmic effects of incomplete ablation lines. It is unknown if a more extensive initial ablation strategy results in improved outcomes following multiple ablation procedures. Methods: 222 consecutive patients with NPAF underwent first-time ablation using a contact-force sensing ablation catheter utilizing either a stepwise (Group 1, n=111) or LA PWI (Group 2, n=111) approach. The duration of follow-up was 36 months. The primary endpoint was freedom from atrial arrhythmia >30s. Secondary endpoints were freedom from persistent arrhythmia, repeat ablation, and recurrent arrhythmia after repeat ablation. Results: There was similar freedom from atrial arrhythmias after index ablation for both stepwise and LA PWI groups at 36 months (60% vs. 69%, p=0.1). The stepwise group was more likely to present with persistent recurrent arrhythmia (29% vs 14%, p=0.005) and more likely to undergo second catheter ablation (32% vs. 12%, p<0.001) compared to LA PWI patients. Recurrent arrhythmia after repeat ablation was more likely in the stepwise group compared to the LA PWI group (15% vs 4%, p=0.003). Conclusions: Compared to a stepwise approach, LA PWI for patients with NPAF resulted in a similar incidence of any atrial arrhythmia, lower incidence of persistent arrhythmia, and fewer repeat ablations. Results for repeat ablation were not improved with a more extensive initial approach.