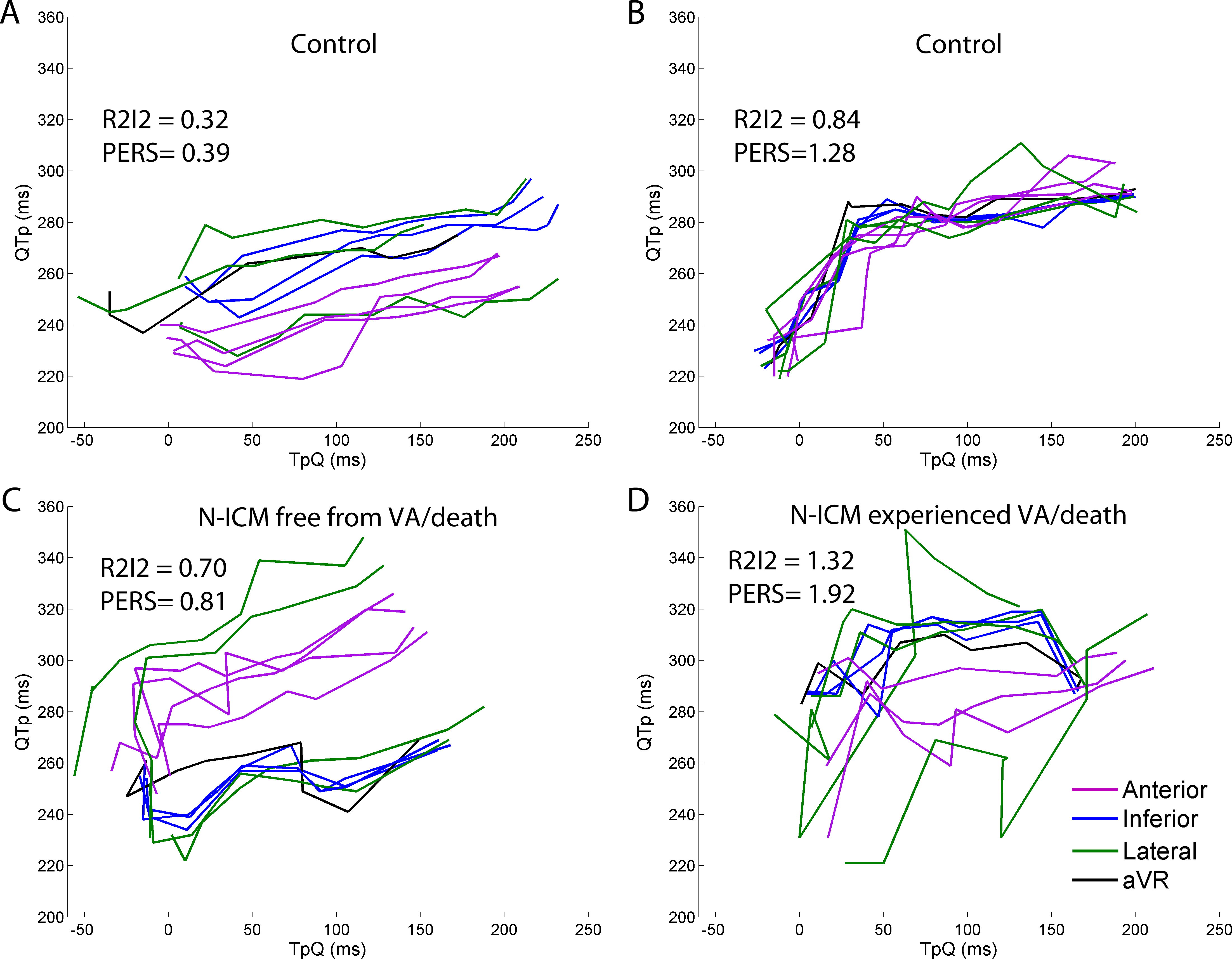
Introduction: Sudden Cardiac Death (SCD) risk assessment is limited, particularly in patients with non-ischemic cardiomyopathies. This is the first application, in patients with non-ischemic cardiomyopathies, of two novel risk markers, Regional Restitution Instability Index (R2I2) and Peak Electrocardiogram Restitution Slope (PERS), which have been shown to be predictive of ventricular arrhythmias (VA) or death in ischemic cardiomyopathy patients. Methods and Results: Blinded retrospective study of 50 patients: 33 dilated cardiomyopathy and 17 other; undergoing electrophysiological study (EPS) for SCD risk stratification, and 29 controls with structurally normal hearts undergoing EPS. R2I2 was calculated from an EPS using ECG surrogates for action potential duration and diastolic interval. Cut-offs for high and low R2I2/PERS were predefined. R2I2 was significantly higher in study than control patients (0.99±0.05 vs. 0.63±0.04, <0.001). PERS showed a trend to higher values in the study group (1.18[0.63] vs. 1.09[0.54], p=0.07). During median follow up of 5.6 years [IQR 1.9 years] 9 study patients reached the endpoint of ventricular arrhythmia(VA)/death. Patients who experienced VA/death showed trends to higher mean R2I2 (1.14±0.07vs.0.95±0.05, p=0.12) and PERS (1.46[0.49] vs. 1.13[0.62], p=0.22). A Cox proportional hazards model using grouped markers: R2I2<1.03+PERS<1.21 / either R2I2≥1.03 or PERS≥1.21 / R2I2≥1.03+PERS≥1.21; significantly predicted VA/death (p=0.02) with a hazard ratio per positive component of 3.2 (95% confidence interval 1.2 to 8.8). Conclusion: R2I2≥1.03+PERS≥1.21 predict VA/death in patients with non-ischemic cardiomyopathies. R2I2≥1.03+PERS≥1.21 have the potential to play an important role in SCD risk stratification in non-ischemic cardiomyopathies but their validity should be confirmed in a larger study.