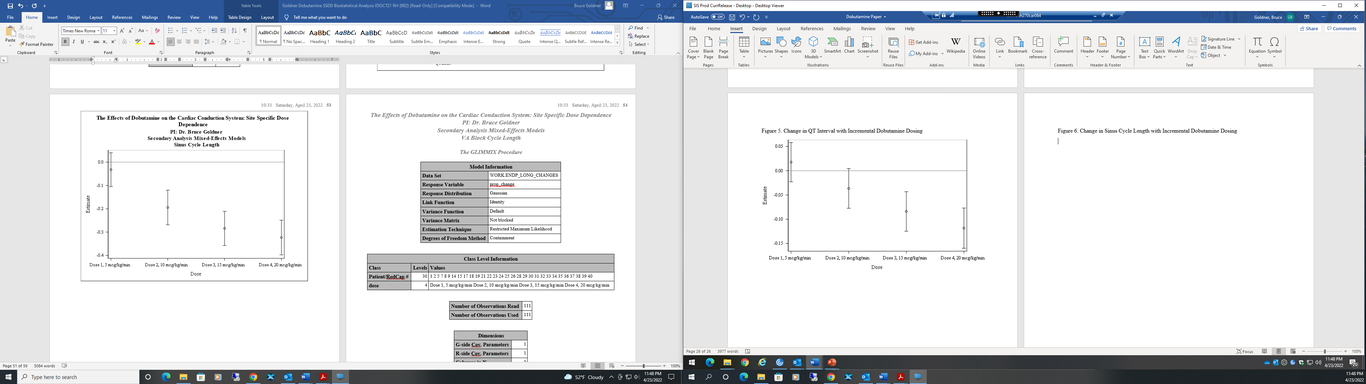
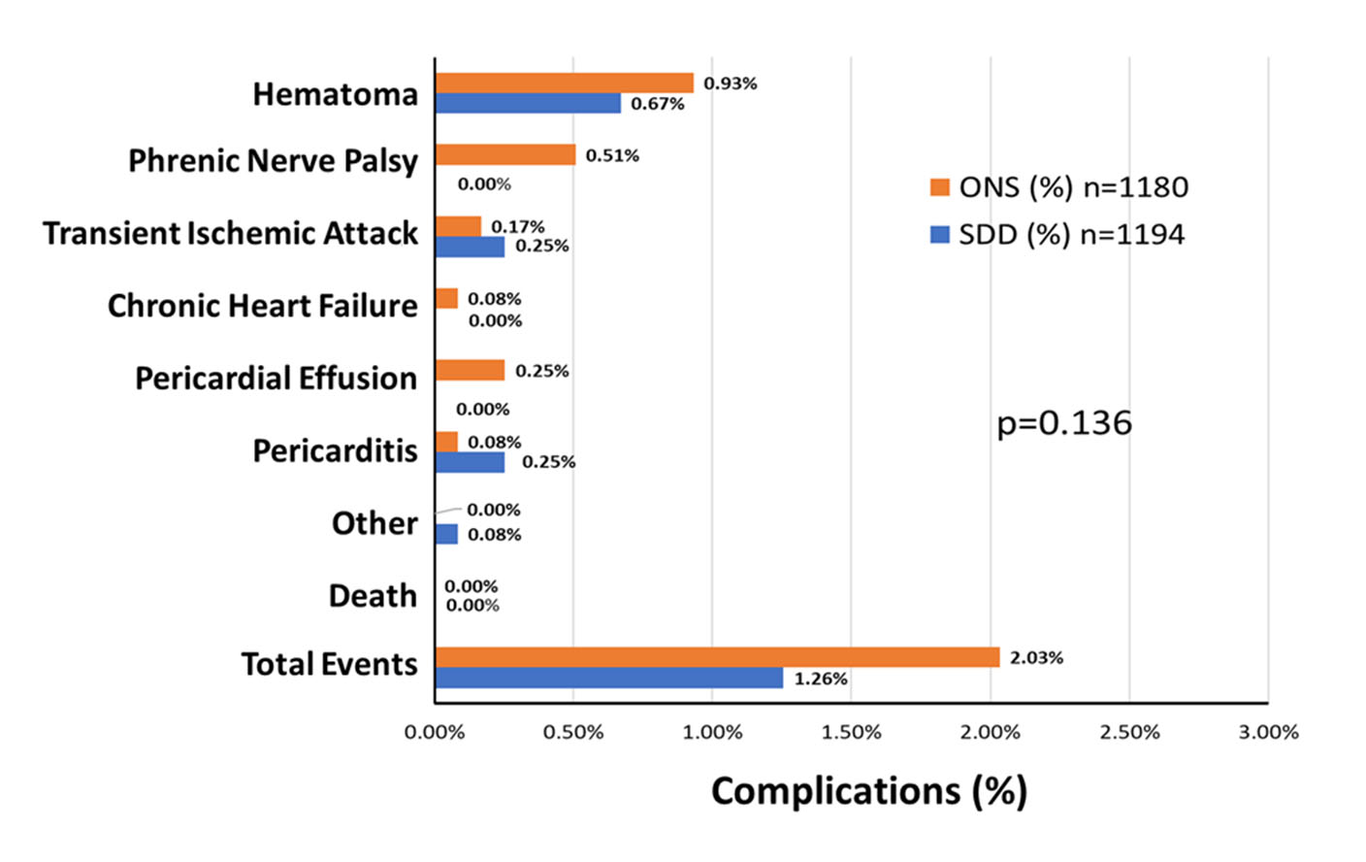
Background: Isoproterenol, a non-specific beta agonist, is commonly used during electrophysiology studies (EPS). However, with the significant increase in the price of isoproterenol in 2015 and the increasing number of catheter ablations performed, the cost implications cannot be ignored. Dobutamine is a less expensive synthetic compound developed from isoproterenol with a similar mechanism to enhance cardiac conduction and shorten refractoriness, thus making it a feasible substitute with a lower cost. However, the use of dobutamine for EPS has not been well-reported in the literature. Objective: To determine the site-specific effects of various doses of dobutamine on cardiac conduction and refractoriness and assess its safety during EPS. Methods: From February 2020 to October 2020, 40 non-consecutive patients scheduled for elective EPS, supraventricular tachycardia, atrial fibrillation, and premature ventricular contraction ablations at a single center were consented and prospectively enrolled to assess the effect of dobutamine on the cardiac conduction system. At the end of each ablation procedure, measures of cardiac conduction and refractoriness were recorded at baseline and with incremental doses of dobutamine at 5, 10, 15, and 20 mcg/kg/min. For the primary analysis, the change per dose of dobutamine from baseline to each dosing level of dobutamine received by the patients, comparing atrioventricular node block cycle length (AVNBCL), ventricular atrial block cycle length (VABCL) and sinus cycle length (SCL), was tested using mixed-effect regression. For the secondary analysis, dobutamine dose level was tested for association with relative changes from baseline of each electrophysiologic parameter (SCL, AVNBCL, VABCL, atrioventricular node effective refractory period (AVNERP), AH, QRS, QT, atrial effective refractory period (AERP), ventricular effective refractory period (VERP), using mixed-effect regression. Changes in systolic and diastolic blood pressures were also assessed. The Holm-Bonferroni method was used to adjust for multiple testing. Results: For the primary analysis there was no statistically significant change of AVNBCL and VABCL relative to SCL from baseline to each dose level of dobutamine. The SCL, AVNBCL, VABCL, AVNERP, AERP, VERP and the AH, and QT intervals all demonstrated a statistically significant decrease from baseline to at least one dose level with incremental dobutamine dosing. Two patients (5%) developed hypotension during the study and one patient (2.5%) received a vasopressor. Two patients (5%) had induced arrhythmias but otherwise no major adverse events were noted. Conclusion: In this study, there was no statistically significant change of AVNBCL and VABCL relative to SCL from baseline to any dose level of dobutamine. As expected, the AH and QT intervals, and the VABCL, VERP, AERP and AVNERP all significantly decreased from baseline to at least one dose level with an escalation in dobutamine dose. Dobutamine was well-tolerated and safe to use during EPS.