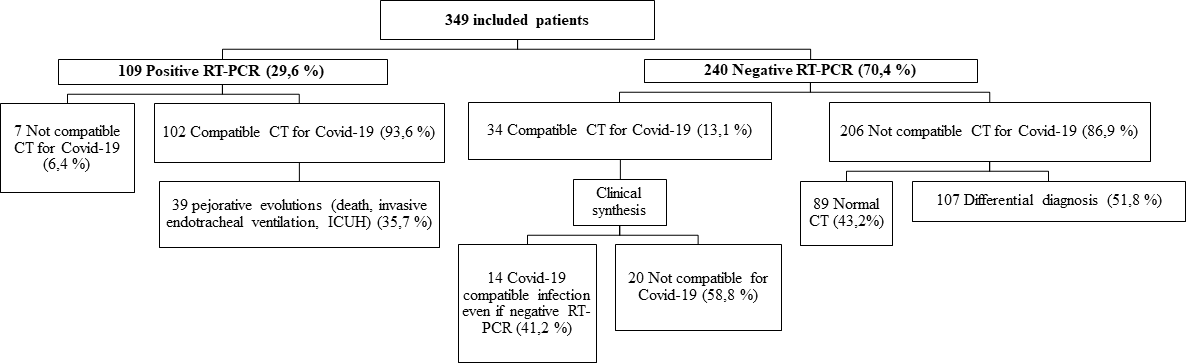
Background COVID-19 is a complex virus that has been spreading since December 2019. In this study, we aimed to assess the association between chest Computed Tomography (CT) signs and pejorative evolution, such as death, use of invasive endotracheal ventilation (IEV) and intensive care unit hospitalization (ICUH). We also evaluated the diagnostic performance of chest CT versus the diagnostic gold standard, RT-PCR. Methods This retrospective monocentric study included 349 patients who had a chest CT either for clinical suspicion of COVID-19 pneumonia with severe initial symptoms, or clinical deterioration in patients with suspected COVID-19 pneumonia, or clinical deterioration in RT-PCR positive patients. Principal judgement criteria for pejorative evolution were: death, IEV, and ICUH. Results Among the 109 RT-PCR positive patients, there were higher rates of bronchial distortion and total volume lung involvement ≥ 50% in the dead, IEV and ICUH groups (p < 10-3). Vascular dilatation and a number of involved lobes ≥ 4 were associated with IEV and ICUH (p < 10-3). Among the 349 patients, sensitivity, specificity, positive and negative predictive values of chest CT versus RT-PCR were respectively 93,6 % [95% CI 89-98,2], 85,8 % [81,4-90,2], 75 % [67,7-82,3], and 96,7 % [94,3-99,1]. Unlike previous studies, we found different kinds of CT signs patterns, rather than a stereotyped COVID-19 pneumonia pattern. Maximal lesion expansion was observed during the second week after the first symptoms. Conclusion Bronchial distorsion and lesion expansion seem to be correlated with death in COVID-19 patients. This study confirms chest CT major diagnostic value.