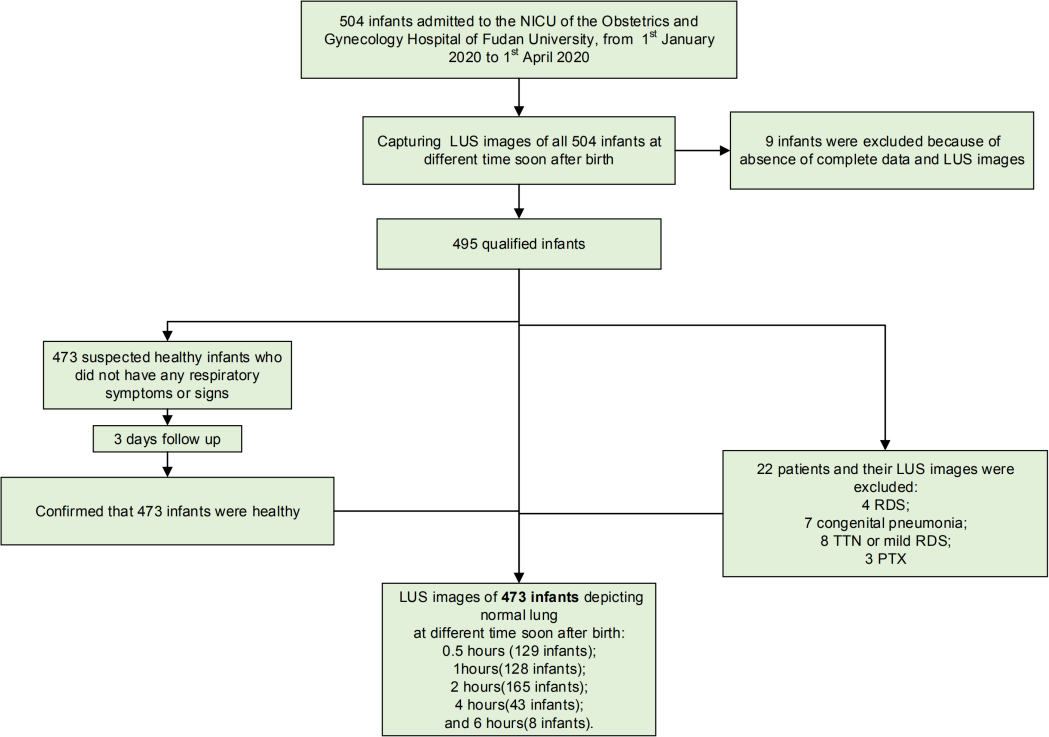
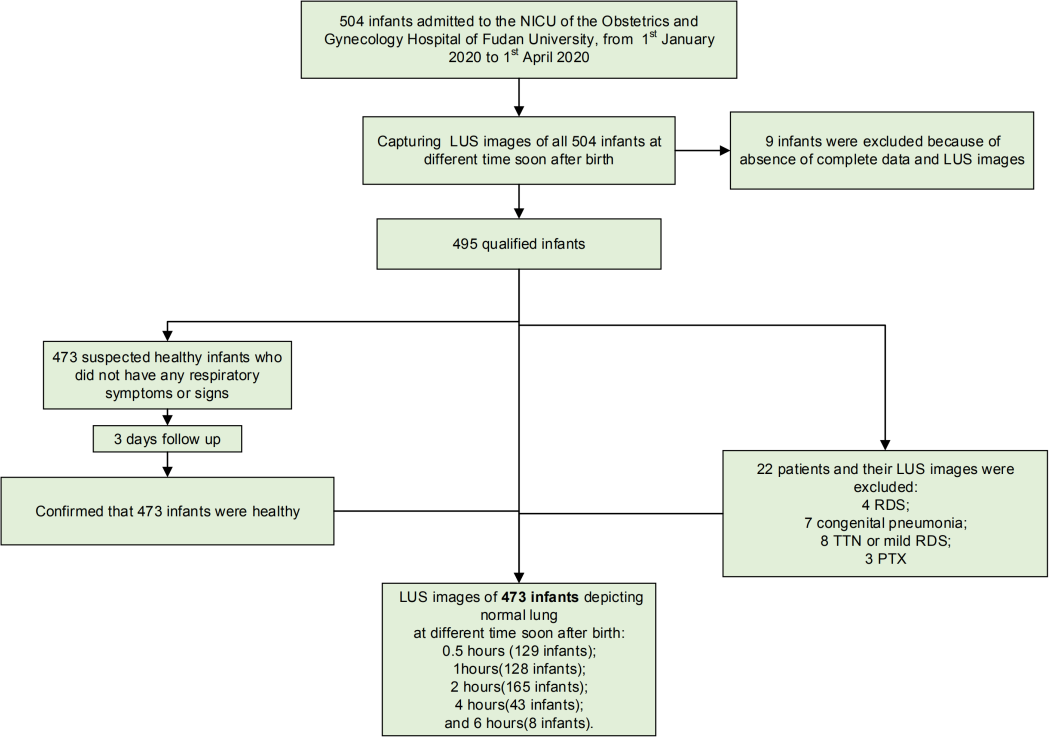
Abstract Background Lung ultrasound (LUS) has been used to diagnose neonatal respiratory diseases. However, few simple method has been reported to predict respiratory support needs(RSN). Our aim was to determine the diagnostic accuracy of a semiquantitative LUS assessment method predicting respiratory support need. Methods We conducted a prospective diagnostic accuracy study following the STARD (Standards for the Reporting of Diagnostic Accuracy Studies) guidelines at a tertiary level academic hospital between 2019 and 2020. After birth, infants were transferred to a monitoring room to determine NICU treatment need. 310 late preterm and term infants with respiratory symptoms enrolled. The LUS assessment was performed for each participant at one of the following times: 0.5 h, 1 h, 2 h, 4 h, and 6 h after birth. Reliability was tested by ROC analysis. Surfactant administration and other RSNs were based on the 2019 European guidelines as well as the infant’s clinical condition. Results 74 have RSN, and 236 were healthy according to a 3-day follow-up confirmation. Six LUS imaging patterns were found. Two “high-risk” patterns were highly correlated with RSN(area under the curve (AUC) = 0.95; 95% CI, 0.92-0.98, p<0.001). This accuracy is supported by the AUC of “low-risk” patterns (0.89, 95% CI, 0.85-0.93, p<0.001). The predictive value of LUS is greater than that of only using respiratory symptoms (e.g., respiratory rate) (AUC of LUS vs AUC of respiratory rate, p<0.01). Conclusions LUS is a useful tool to predict RSN and is more reliable than assessments based on respiratory symptoms alone.