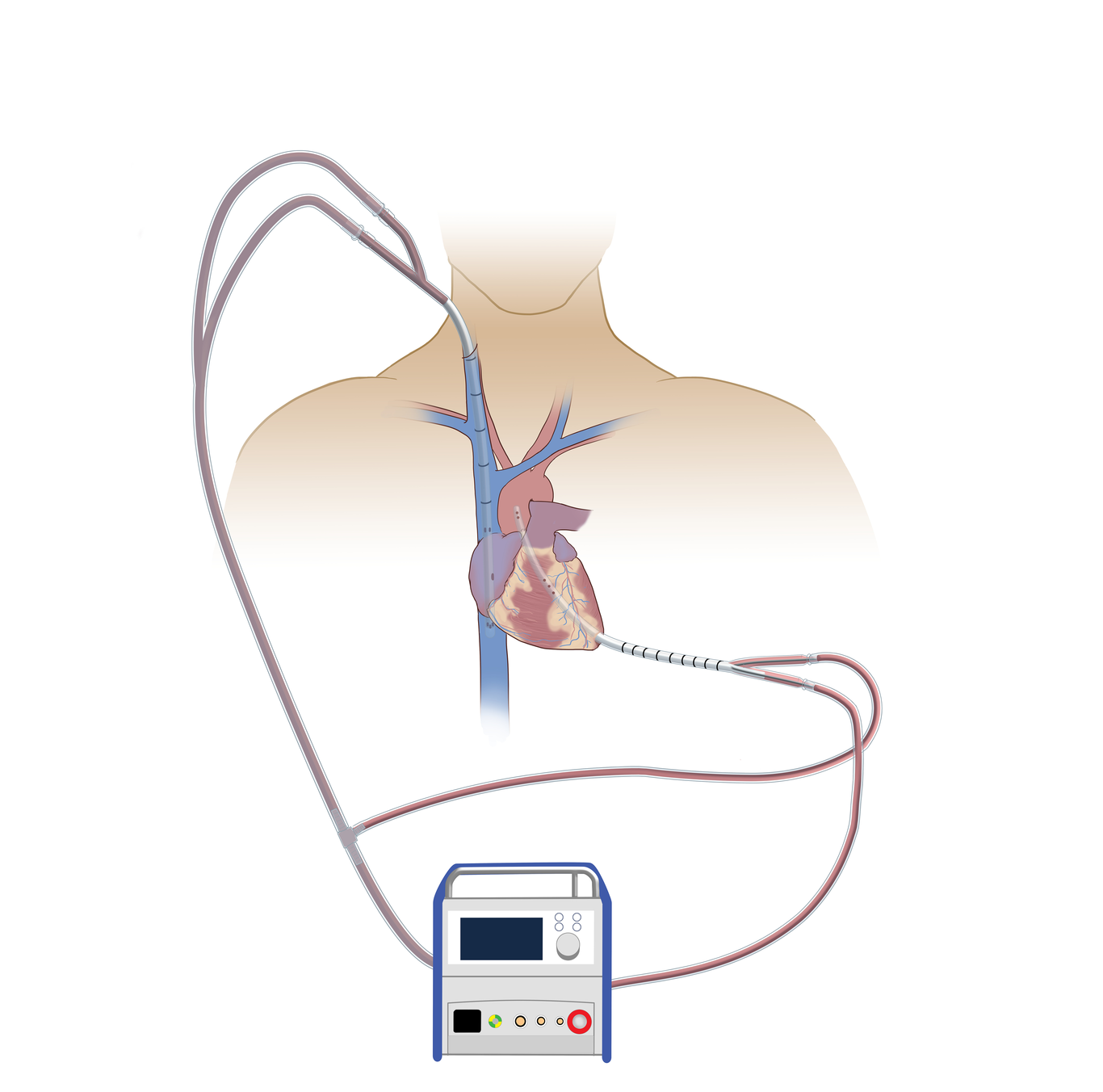
Fulminant myocarditis is a rapidly progressive myocardial inflammation that commonly requires advanced therapies circulatory support. We report our management for a case of fulminant myocarditis and cardiogenic shock. The patient is a 36 year old gentleman who was admitted after a one week history of malaise. Upon admission he was lethargic with jugular venous distension to 10 cm. He was taken immediately for a heart catheterization and intra-aortic balloon pump placement. There was no obstructive coronary disease, and hemodynamics were consistent with biventricular failure. After multidisciplinary evaluation, we elected to proceed with emergent extracorporeal membranous oxygenation (ECMO). We utilize a Protek Duo Rapid Deployment (LivaNova, Mirandola, Italy) which is inserted via modified Seldinger technique through the left ventricular apex, terminating in the ascending aorta. Percutaneous right IJ bicaval via a y-ed Avalon Elite (Getinge, Goteborg, Sweden) approach is employed for venous drainage (Figure 1). We believe that with this alternative ECMO cannulation platform, we address the multitude of drawbacks that plague peripherally cannulated extracorporeal circulatory support, minimizing patient deconditioning and upper/lower extremity over/under perfusion complications, while providing sternal sparring antegrade arterial flow with ventricular unloading/venting. For two weeks the patient was ambulatory, but because we were unable to obtain an adequate offer during this interval, we transitioned to a bridge to bridge therapy. This case highlights an alternate strategy for central walking VA ECMO in the rare presentation of one patient’s progression from IABP to VA ECMO to durable BiVAD to heart transplantation during a single admission.