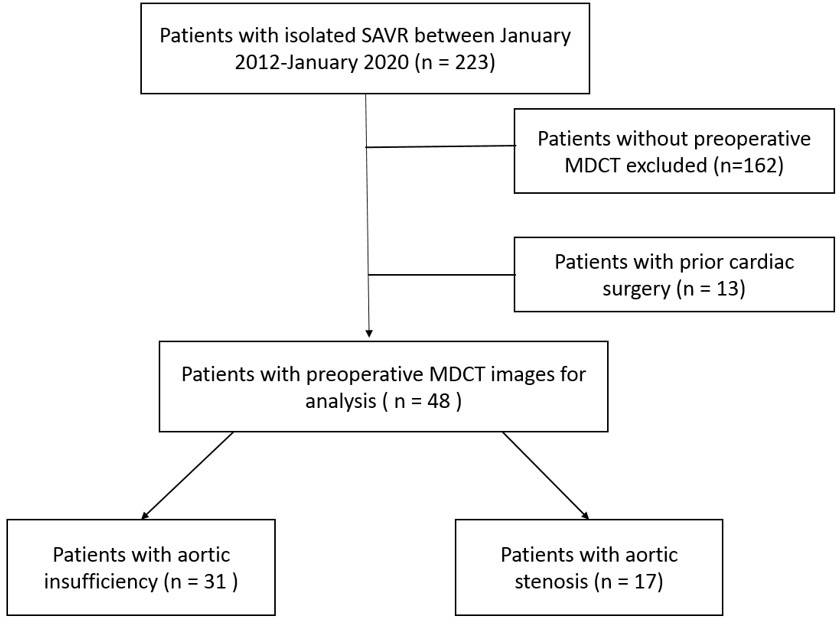
ABSTRACT: Background: Valve-in-valve (ViV) transcatheter aortic valve replacement (TAVR) has become a valuable option in patients with bioprosthetic failure. However, potential issues with ViV TAVR may occur in patients with high risk anatomy for coronary obstruction and patients with baseline smaller bioprosthetic valves at risk for patient prosthesis mismatch. The purpose of this study was therefore to use preoperative electrocardiography (ECG)-gated, multidetector computed tomography (MDCT) in patients undergoing isolated surgical aortic valve replacement (SAVR) to 1) identify which would be high risk for coronary occlusion with ViV TAVR, and 2) predict intraoperative SAVR sizing. Methods: Among 223 patients from our institutions’ database that underwent SAVR for aortic insufficiency (AI) or aortic stenosis (AS) between January 2012 and January 2020, 48 patients had MDCT imaging prior to surgery (AI; n=31, AS; n=17). Of all patients, 67% (n=32) were bicuspid morphology. Results: With the use of virtual valve implantation, all patients with AI and bicuspid AS had feasible anatomy for ViV TAVR, while 38% of patients with tricuspid AS were high risk for coronary obstruction. There was a strong correlation between actual valve size implanted and preoperative MDCT measurements using annulus average diameter, area and/or perimeter. Conclusion: Preoperative MDCT in patients undergoing SAVR is a useful tool for lifetime management, particularly in patients with tricuspid AS. Decisions for surgical management may change based on MDCT’s ability to predict intraoperative SAVR size and determine which patients may be high risk candidates for future ViV TAVR due to coronary artery obstruction.