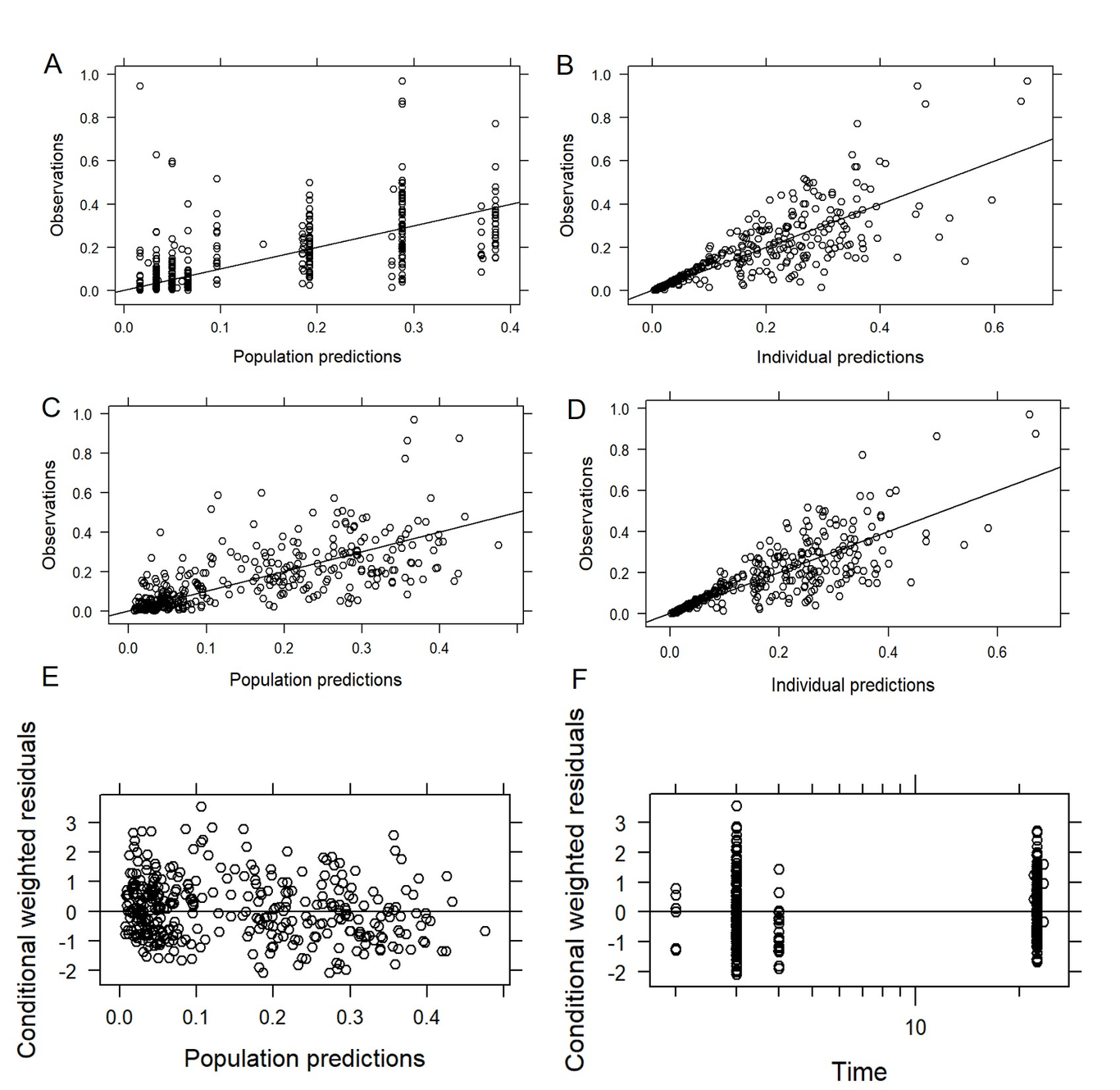
Aim: The aim of this study was to establish a population pharmacokinetic (PPK) model for rivaroxaban in Chinese elderly patients with NVAF to evaluate precision dosing regimens and analyze hemorrhagic risk after rivaroxaban treatment. Method: A population pharmacokinetic model was developed using the nonlinear mixed-effects model (NONMEM). The plasma concentration of rivaroxaban was detected by UPLC-MS/MS method and the gene polymorphisms were detected by Sanger dideoxy DNA sequencing method. A Monte Carlo simulation was performed to evaluate various dosing schemes and different levels of covariates for the target range of therapeutic drug monitoring concentrations (Cmax,ss, Cmin,ss). Exposure of rivaroxaban was simulated and assessed in hemorrhagic risk evaluation. Results: Model-building dataset including 360 plasma concentrations from 180 Chinese elderly patients (median age 81year). A one-compartment population PK model with estimated glomerular filtration rate (eGFR), total bilirubin (TBIL) and ABCB1 rs1045642 as major covariates for apparent clearance were developed. The average probability of target attainment (PTA) of optimal dosing regimens with different covariates levels for targeted Cmax,ss and Cmin,ss were 29.35%-31.30% and 64.91%-65.80%, respectively. 10 mg of rivaroxaban in Chinese elderly patients with normal renal and liver function was appropriate. AUC24,ss was statistically significant associated with the increased risk of the bleeding events (OR 1.0006; 95%CL 1.0003-1.001; p<0.0001). Conclusion: Lower dose is recommended for older patients with renal impairment to avoid overexposure and bleeding events. The population pharmacokinetic model could inform individualized dosing for Chinese older NVAF patients with rivaroxaban anticoagulation therapy.