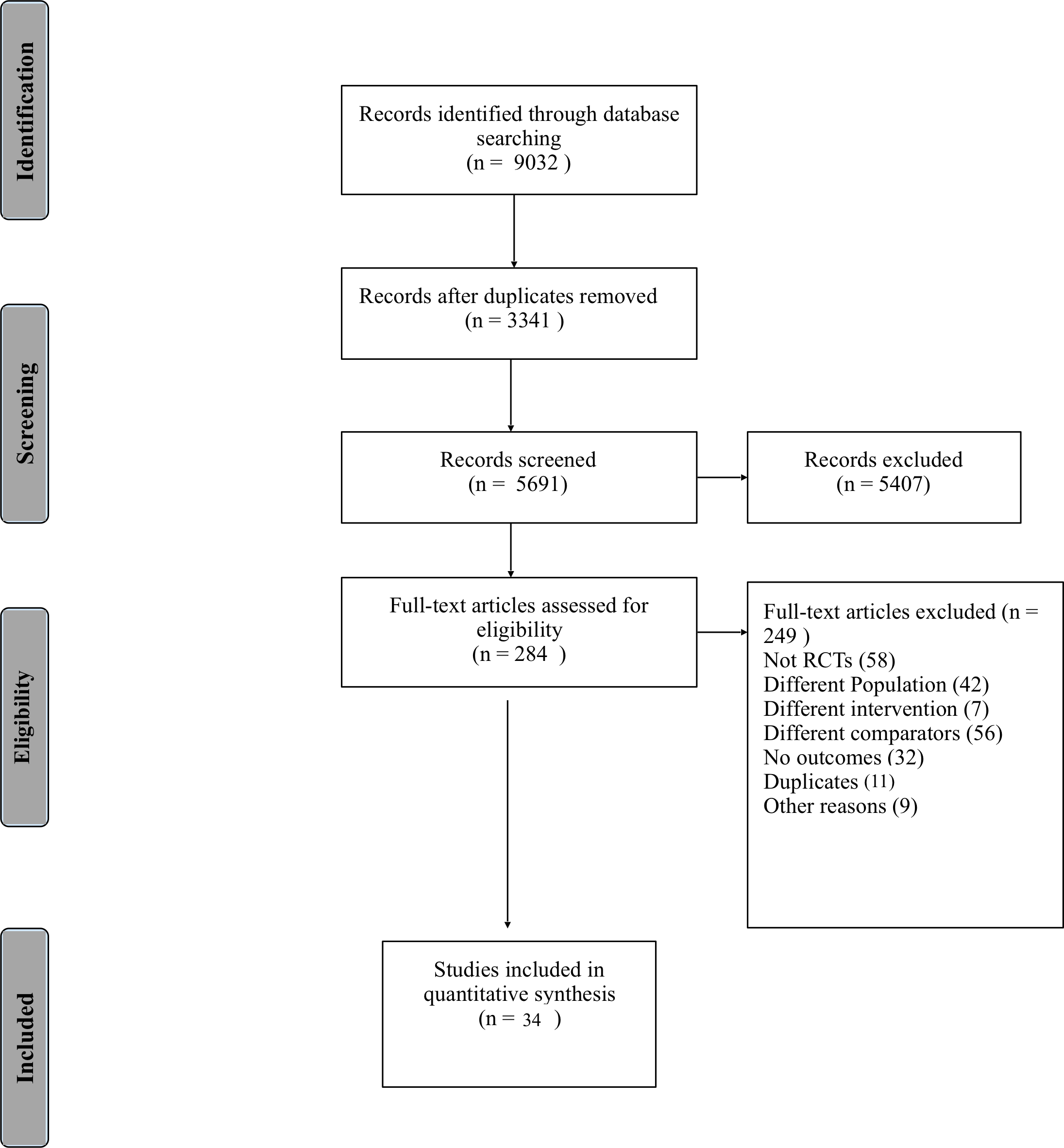
Objectives: To compare the efficacy of different non-invasive respiratory support modes for primary respiratory support of preterm infants with Respiratory Distress Syndrome (RDS). Design: Systematic review and network meta-analysis using the Bayesian random effects approach. MEDLINE, EMBASE and CENTRAL were searched. Interventions : HFNC (High Flow Nasal Cannula), CPAP (Continuous Positive Airway Pressure), BiPAP (Bilevel CPAP), NIPPV (Non Invasive Positive Pressure Ventilation). Main outcome measures: Requirement of invasive mechanical ventilation, any treatment failure. Results: 34 studies including 3994 patients were included. NIPPV was more effective in decreasing the requirement of mechanical ventilation than CPAP {RR [95% Credible Interval (CrI)] - 0.60 (0.44, 0.79)}and HFNC [0.66 (0.43, 0.99)]. Surface under the cumulative ranking curve (SUCRA) for NIPPV, BiPAP, HFNC and CPAP were 0.94, 0.59, 0.32 and 0.13. For the outcome of treatment failure, both NIPPV and BiPAP were more efficacious compared to CPAP and HFNC {0.56 (0.44, 0.71) [NIPPV vs CPAP], 0.69 (0.51, 0.93) [BiPAP vs CPAP], 0.42 (0.30, 0.63) [NIPPV vs HFNC], 0.53 (0.35, 0.81) [BiPAP vs HFNC]}. The SUCRA for NIPPV, BiPAP, CPAP and HFNC were 0.96, 0.70, 0.32 and 0.01. NIPPV was associated with a reduced risk of air leak compared to BiPAP and CPAP [0.36 (0.16, 0.73); 0.54(0.30, 0.87), respectively]. NIPPV resulted in lesser incidence of BPD or mortality when compared to CPAP [0.74 (0.52, 0.98)]. Nasal injury was lesser with HFNC compared to CPAP [0.15 (0.01, 0.60)]. Conclusions: Most effective primary mode of non-invasive respiratory support in preterm neonates with RDS was NIPPV.