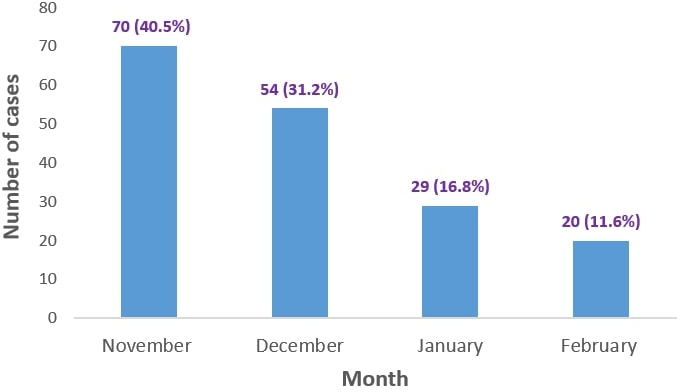
Objectives: To describe clinico-virological profile, treatment details, intensive care needs, and outcome of infants with acute viral bronchiolitis (AVB). Methodology: In this prospective study, 173 infants with AVB admitted to Pediatric emergency and Pediatric intensive care unit (PICU) of a tertiary care teaching hospital in North India during November 2019 to February 2020 were enrolled. The data collection included clinical features, viruses detected, complications, intensive care needs, treatment, and outcome. Multivariate analysis was performed to determine independent predictors for PICU admission. Results: Patients had rapid breathing (98.8%), cough (98.3%), and fever (74%). On examination, tachypnea (98.8%), chest retractions (93.6%), respiratory failure (84.4%), wheezing (49.7%), and crepitations (23.1%) were observed. RSV and rhinovirus were predominant isolates. Complications were noted in 25% cases as encephalopathy (17.3%), transaminitis (14.3%), shock (13.9%), AKI (7.5%), myocarditis (6.4%), MODS (5.8%), and ARDS (4.6%). More than one-third cases required PICU admission requiring nasal cannula oxygen (11%), continuous positive airway pressure (51.4%), high flow nasal canula (14.5%), and mechanical ventilation (23.1%); nebulization (74%); antibiotics (35.9%); and vasoactive drugs (13.9%). The mortality was 8.1%. Underlying comorbidity; chest retractions, respiratory failure, and low oxygen saturation at admission; presence of shock; and need of mechanical ventilation were independent predictors of PICU admission. Isolation of virus or co-infection were not associated with disease severity, intensive care needs, and outcome. Conclusion: Among infants with AVB, RSV and rhinovirus were predominant; >1/3rd required PICU admission; and comorbidity; chest retractions, respiratory failure, low oxygen saturation; shock; and need of mechanical ventilation independently predicted PICU admission.