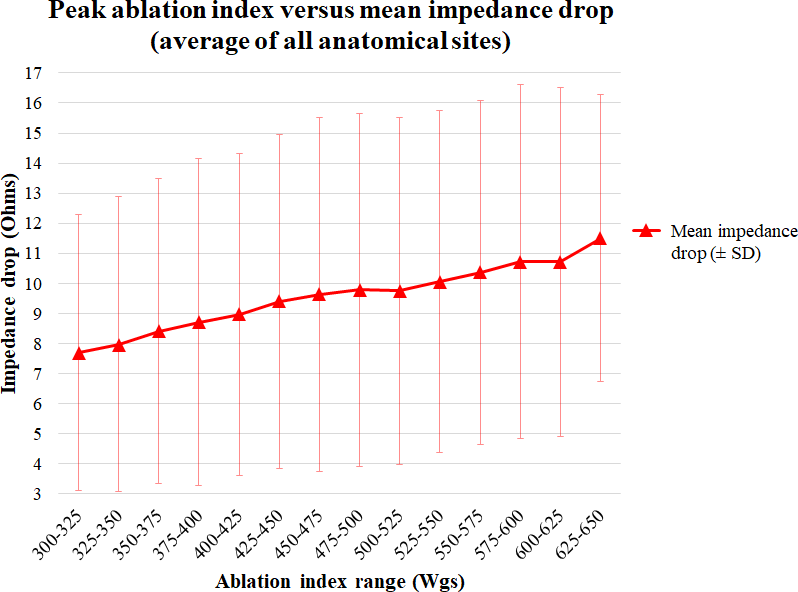
Introduction Anatomical studies demonstrate significant variation in cavotricuspid isthmus (CTI) architecture. We hypothesised that ablation index (AI) may further our understanding of energy delivery across the CTI. Methods 38 patients underwent CTI ablation at two Cardiothoracic hospitals. Operators delivered 682 lesions in total with a target AI of 600Wgs. Ablation parameters were recorded every 10-20ms. Post hoc, Visitags were trisected according to CTI position: inferior vena cava (IVC), middle (Mid), or ventricular (V) lesions. Results There were no complications. 97.4% of patients (n=37) remained in sinus rhythm at 6.6±3.3 months’ follow-up. For the whole CTI, peak AI correlated with mean impedance drop (ID) (R2=0.89, p<0.0001). However, analysis by anatomical site demonstrated a non-linear relationship Mid CTI (R2=0.15, p=0.21). Accordingly, whilst mean AI was highest Mid CTI (IVC: 473.1±122.1 Wgs, Mid: 539.6±103.5 Wgs, V: 486.2±111.8 Wgs, ANOVA p<0.0001), mean ID was lower (IVC: 10.7±7.5Ω, Mid: 9.0±6.5Ω, V: 10.9±7.3Ω, p=0.011), and rate of ID was slower (IVC: 0.37±0.05 Ω/s, Mid: 0.18±0.08 Ω/s, V: 0.29±0.06 Ω/s, p<0.0001). Mean contact force was similar at all sites, however temporal fluctuations in contact force (IVC: 19.3±12.0mg/s, Mid: 188.8±92.1mg/s, V: 102.8±32.3mg/s, p<0.0001) and catheter angle (IVC: 0.42°/s, Mid: 3.4°/s, V: 0.28°/s, p<0.0001) were greatest Mid CTI. Use of a long sheath attenuated these fluctuations and improved ablation efficacy. Conclusions Ablation characteristics vary across the CTI. At the Mid CTI, operators should appreciate that higher AI values do not necessarily deliver more effective ablation; this may be explained by localised fluctuations in catheter angle and contact force.