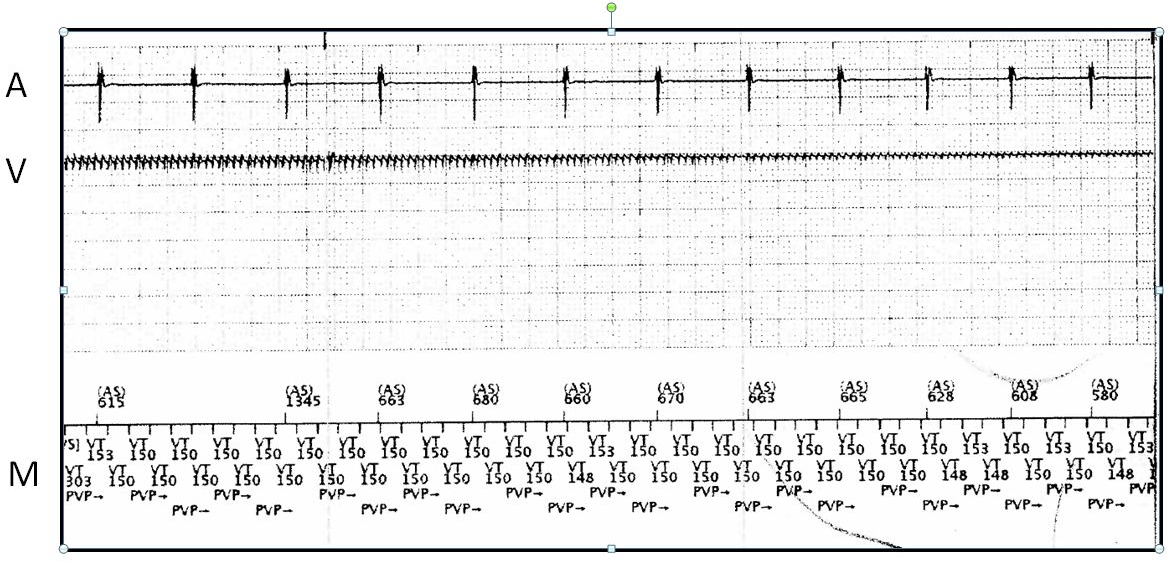
Case PresentationA 62 year old man with a past medical history of hypertension and mild coronary artery disease underwent dual chamber permanent pacemaker (PPM) implantation in April of 2015 for complete heart block. A Boston Scientific Ingenio K173 (Boston Scientific, St. Paul, MN) generator was inserted and connected to 2 Medtronic 5076 pacing leads (Medtronic, Minneapolis, MN) which were positioned in the right atrium (RA) and right ventricle (RV). The operative report noted “normal testing results” with an acute RV lead bipolar pacing threshold of 0.6 V at 0.4 msec and pacing impedance of 550 Ω. The PPM was programmed DDDR 60-130 bpm with RA and RV lead outputs programmed 3 times threshold.He had no further syncope after implant but continued to complain of intermittent lightheadedness as soon as a week out from the implant. Multiple pacemaker interrogations revealed stable atrial and ventricular lead function and he was told that his symptoms were likely due to low blood pressure which resulted in his blood pressure medicines being adjusted. The patient presented to his local hospital with recurrent syncope without warning 14 months after the initial implant. PPM interrogation recorded noise resulting in RV pacing inhibition (Figure 1). RV bipolar lead pacing threshold was 0.6 V at 0.4 msec and the pacing impedance measured 660 Ω. Historical RV lead pacing threshold and impedance trends were stable. RV lead oversensing was suspected and pocket manipulation, deep inspiration, Valsalva maneuver, arm isometrics, left arm extension, abduction and adduction did not duplicate the noise. The device was reprogrammed to asynchronous mode (DOO at 80 bpm) and the patient was transferred to our hospital for lead extraction.After confirming the interrogation findings, a chest radiograph was performed which showed no obvious fracture, gross dislodgement or lead discontinuity. What is the likely cause of the noise on the RV lead and this patient’s recurrent syncopal episodes?