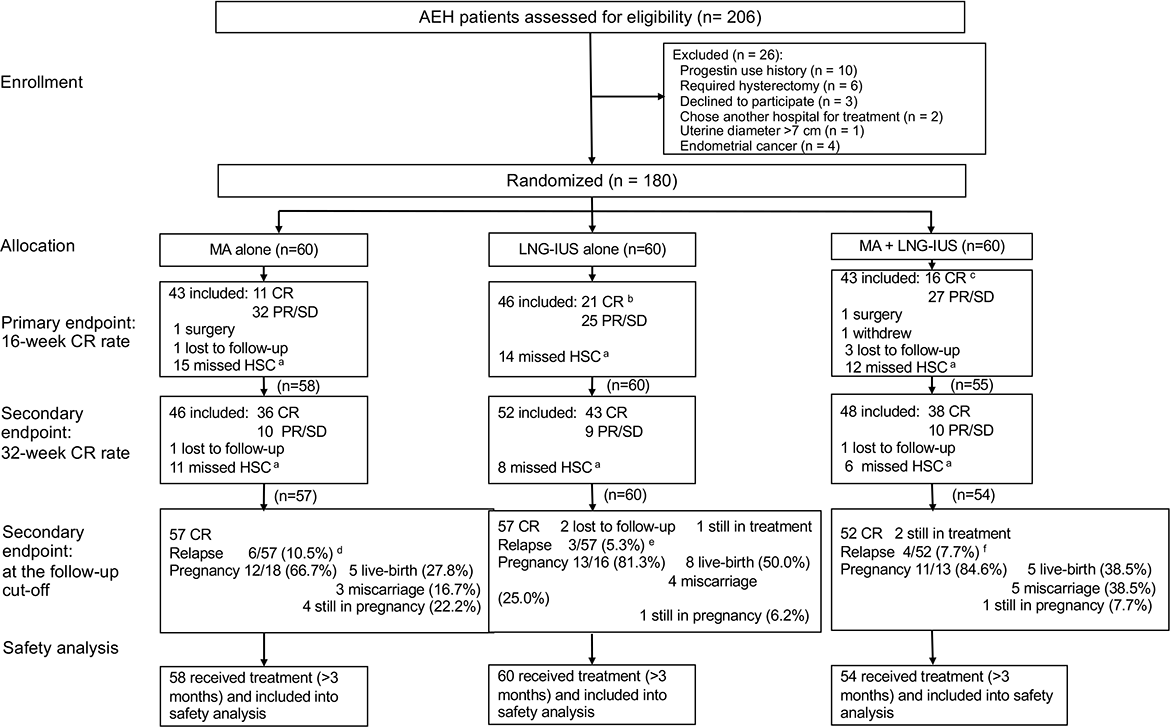
Objective To compare the effect of levonorgestrel-intrauterine system (LNG-IUS) with or without oral megestrol acetate (MA) versus MA alone on fertility preserving treatment in patients with atypical endometrial hyperplasia (AEH). Design Single-center phase II study with open-label, randomized and controlled trial conducted between July 2017 and June 2020. Setting Obstetrics & Gynecology Hospital of Fudan University, Shanghai, China Population A total of 180 patients (18-45 years) with primary AEH were randomly assigned (1:1:1) to MA group (N=60), LNG-IUS group (N=60), or MA+LNG-IUS group (N=60). Methods Patients received MA (160 mg orally daily), LNG-IUS, or MA+LNG-IUS (MA 160 mg orally daily plus LNG-IUS), respectively. Main outcomes and measures The primary endpoint was the complete response (CR) rate at 16 weeks of treatment. The secondary endpoints were the CR rate at 32 weeks of treatment, adverse events, recurrent rate, and pregnancy rate. Results LNG-IUS group yielded a higher 16-week CR rate than MA group (P=0.049; Odds ratio [OR], 2.44; 95% confidence interval [95%CI], 1.00-6.00). However, MA+LNG-IUS group did not yield better 16-week or 32-week CR rates than MA group (P=0.245; P=0.915) or LNG-IUS group (P=0.419; P=0.653). Meanwhile, less side-effects were found in LNG-IUS group compared with the other two groups. No significant difference was seen in recurrence rates and pregnancy rates among all three groups. Conclusions LNG-IUS might be considered as the first-line choice of fertility-sparing treatment in AEH patients with proper size of uterine cavity. LNG-IUS combined with MA might not provide better treatment effect than MA or LNG-IUS alone.