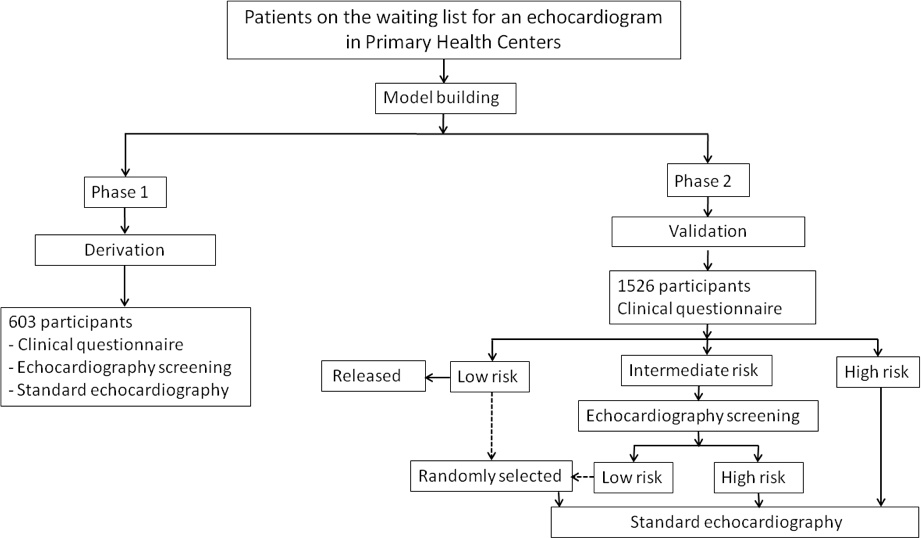
Introduction: Access to public healthcare is limited in Brazilian underserved areas, and long waiting lists remain for echocardiography (echo). We aimed to develop a tool to optimize indications and shorten waiting lists for standard echo in primary care. Methods: Patients in waiting list for standard echo were enrolled. For derivation, patients underwent a clinical questionnaire, simplified 7-view echo screening by non-physicians with handheld devices (GE-VSCAN), and standard echo (Vivid-Q) by experts. Two models were adjusted, one including clinical variables and other adding screen-detected major heart disease (HD). For validation, patients were risk-classified according to the clinical score. High-risk patients and a sample of low-risk underwent standard echo. Intermediate-risk patients first had screening echo, with a complete study if HD was suspected. Discrimination and calibration of the 2 models were assessed to predict HD in standard echo. Results: In derivation (N=603), clinical variables associated with HD were female gender, body mass index, Chagas disease, prior cardiac surgery, coronary disease, valve disease, hypertension, and heart failure, and this model was well calibrated with C-statistic=0.781. Performance was improved with the addition of echo screening, with C-statistic=0.871 after cross-validation. For validation (N=1,526), 227 (14.9%) patients were classified as low-risk, 1082 (70.9%) as intermediate-risk, and 217 (14.2%) as high-risk by the clinical model. The final model with 2 categories had high sensitivity (99%) and negative predictive value (97%) for HD in standard echo. Model performance was good with C-statistic=0.720. Conclusion: The addition of screening echo to clinical variables significantly improves the performance of a score to predict major HD.