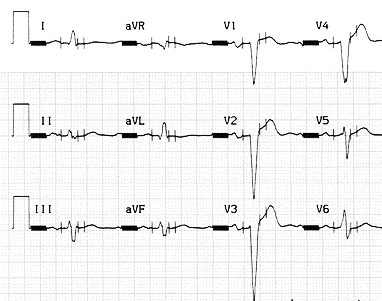
Under psychological stress, a 61-year-old man fainted and quickly regained consciousness, but with a slight head injury. He did not complain of symptoms when he exercised, but was not really physically active. Fifteen years ago, he had a myocardial infarction, then two years later, was diagnosed with congestive heart failure. Three years ago, he underwent a coronary angiography procedure. It showed occlusion of the left descending coronary artery and mild stenosis of the right coronary artery. Stress myocardial scintigraphy showed no ischemic areas requiring a revascularization procedure.Baseline electrocardiogram (ECG) showed first-degree atrioventricular block and incomplete left bundle branch block. Severe dilation of the left ventricle was observed on the echocardiogram (end-diastolic diameter = 87 mm, ejection fraction = 0.24).In order to rule out further damage to the coronary arteries, an exercise test was performed using a 30W/3min-step protocol. At the 60W step, the ECG showed sinus tachycardia with QRS widening from 120 to 160 msec (fig. 1A-1B). Although the test was stopped, a wide QRS tachycardia occurred. The patient briefly fainted, with complete regaining of consciousness in the supine position. The tachycardia rate was 155 bpm, with a left bundle branch block pattern and left-axis deviation (fig. 1C).Atrioventricular dissociation was likely to be present on lead V1, consistent with ventricular tachycardia. What could be the mechanism responsible for this tachycardia ?