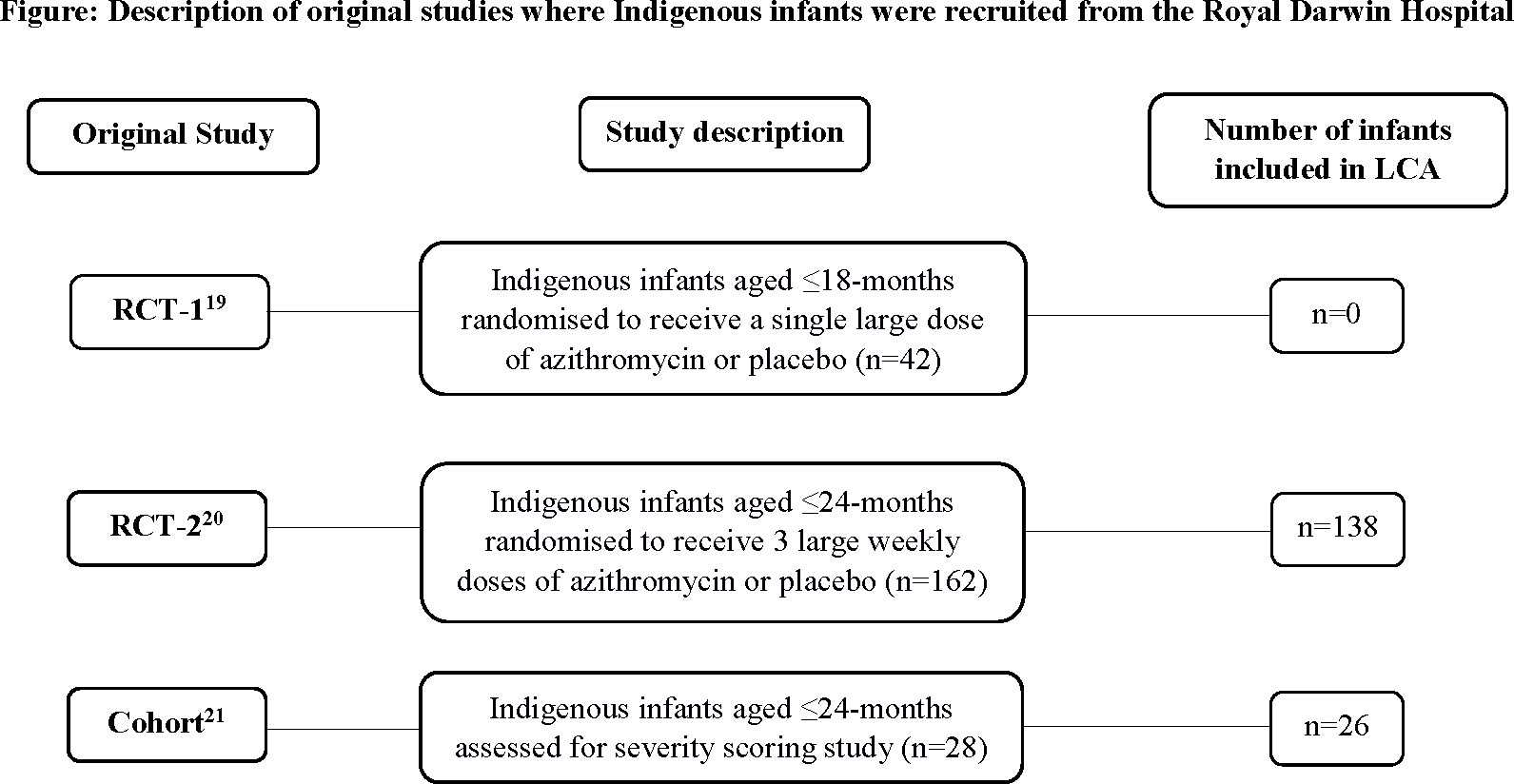
Abstract Background and Objectives: Better phenotyping of the heterogenous bronchiolitis syndrome may lead to targeted future interventions. This study aims to identify severe bronchiolitis profiles among hospitalised Australian Indigenous infants, a population at high-risk of bronchiectasis, using Latent Class Analysis (LCA). Methods: We included prospectively collected clinical, viral and nasopharyngeal bacteria data from 164 Indigenous infants hospitalised with bronchiolitis. We undertook multiple correspondence analysis (MCA) followed by LCA. The best-fitting model for LCA was based on adjusted Bayesian information criteria and entropy R2. Results: We identified five clinical profiles. Profile-A’s (23.8% of cohort) phenotype was previous preterm (90.7%), low birth-weight (89.2%) and weight-for-length z-score <-1 (82.7% from combining those with z-score between -1 and -2 and those in the z-score of <-2 group) previous respiratory hospitalisation (39.6%) and bronchiectasis on chest high-resolution computed tomography scan (35.4%). Profile-B (25.3%) was characterised by oxygen requirement (100%) and marked accessory muscle use (45.5%). Infants in profile-C (7.0%) had the most severe disease, with oxygen requirement and bronchiectasis in 100%, moderate accessory muscle use (85% vs 0-51.4%) and bacteria detected (93.1% vs 56.7-72.0%). Profile-D (11.6%) was dominated by rhinovirus (49.4%), mild accessory muscle use (73.8%) and weight-for-length z-score <-2 (36.0%). Profile-E (32.2%) included bronchiectasis (13.8%), RSV (44.0%), rhinovirus (26.3%) and any bacteria (72%). Conclusions: Using LCA in Indigenous infants with severe bronchiolitis, we identified 5 clinical profiles with one distinct profile for bronchiectasis. LCA can characterise distinct phenotypes for severe bronchiolitis and infants at risk for future bronchiectasis, which may inform future targeted interventions.