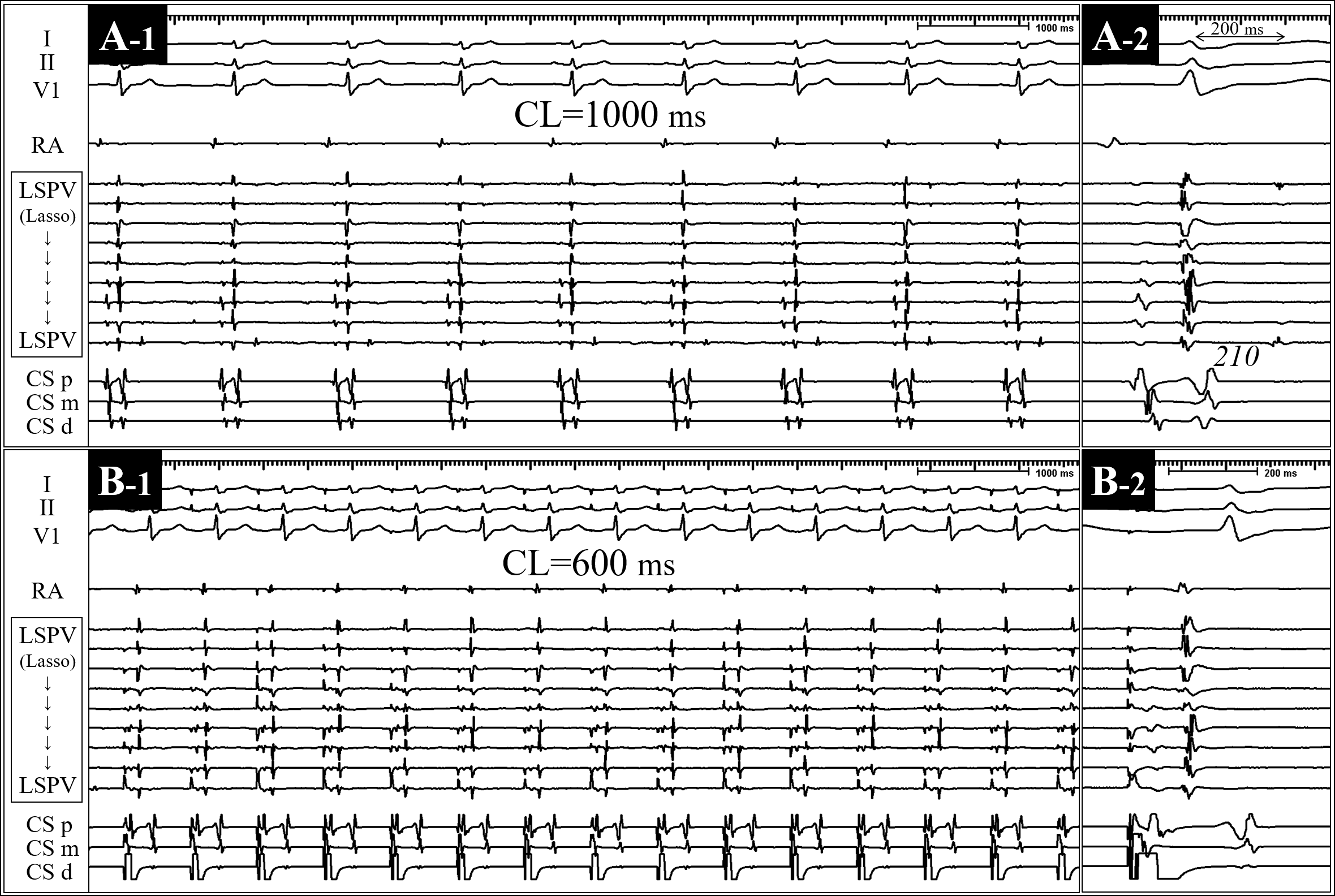
CASE PRESENTATION: A 70-year-old man with drug refractory symptomatic paroxysmal atrial fibrillation (AF) was referred for pulmonary vein isolation (PVI). After completing anatomical PV encirclement, interrogation of the PVs with a circular mapping catheter (CMC) showed that left superior PV (LSPV) remained electrically connected (entrance block into left inferior PV was confirmed). Body surface ECG and intracardiac electrograms during sinus rhythm [sinus cycle length (CL), 1000 ms] (figure 1-A) and during pacing from distal coronary sinus (CS) at a CL of 600 ms are shown (figure 1-B). When the pacing CL was lengthened to 750 ms, atrial trigeminy appeared with a fixed coupling interval (figure 2). The trigeminy vanished when pacing CL was 700, 800, and 900 ms (data not shown), however, it was reproducibly induced only when pacing CL was 750 ms.What is the mechanism of the atrial trigeminy induced only at the specific pacing CL?COMMENTARIES:During sinus rhythm, the 2 distinct PV potentials (P1 and P2) were recorded on the CMC placed within the LSPV ostium (figure 1-A). The interval between P1 and P2 was 210 ms during sinus. When pacing at the CL of 600 ms from the distal CS, however, the P2 disappeared (figure 1-B). When the pacing CL is increased up to 750 ms, not only the P2 appeared again, but also the P1-P2 interval presented a Wenckebach periodicity increasing slightly from 235 to 245 ms (figure 3-A). Moreover, the third PV potential (P3) appeared every third beat and was conducted to the left atrium (LA), resulting in the atrial trigeminy. The P1-P3 interval was constant (245+135 ms), which led to the fixed coupling interval. The third pacing impulse did not capture the LA which remained refractory (figures 2 and 3-A).Then, what is the mechanism of the double or triple PV responses to a single atrial impulse? The P1 and P3 were recorded on the all bipoles of the CMC but they were different in activation sequence [note the site of earliest PV spike of each PV potential (arrows in figure 3-A)]. Whereas, the P2 was recorded only on limited bipoles of the CMC, suggesting far-field signals from the distal LSPV. These findings indicated that the P3 was an “echo” from the distal LSPV. The reproducible induction of the PV echo by atrial stimulation at the specific pacing CL indirectly suggested reentry as its mechanism.Proposed mechanism of the intra-PV reentry causing the echoes is demonstrated in Figure 3-B. Two PV myocardial sleeves which meet the following criteria are assumed: 1) each of the 2 sleeves remains connected to the left atrium (LA); 2) one of the 2 sleeves has a slower conduction velocity and a slightly longer refractory period than the other (“faster” and “slower” sleeves); and 3) the 2 sleeves are connected at the site distal to the slow conduction zone existing between the proximal and distal PVs. When the pacing CL was 600-700 ms, P2 (represents depolarization of distal PV sleeve) was not produced since the slow conduction zone was refractory (figure 3-B1). When the pacing CL was 750-1000 ms, the P2 was produced via the faster sleeve. P3 was not present since retrograde impulse from the faster sleeve was blocked within the slower sleeve due to refractoriness or collision with impulse via the slower sleeve (figure 3-B2). When the pacing CL was 750 ms, both the P2 and P3 appeared since unidirectional block occurred in the slower sleeve, and the P3 was conducted to the LA (figure 3-B3). Almost no difference in length of refractory period of the two PV sleeves may have resulted in the very narrow echo zone.After the radiofrequency application at the anterior carina of the LSPV, which resulted in entrance block into the LSPV, the PV echo was no longer inducible despite pacing within the PV or provocative isoproterenol and adenosine. The patient is currently asymptomatic 1 year after the procedure, with no evidence of AF recurrence.In the present case, an uncommon cause of atrial trigeminy; atrial impulse-triggered PV echo associated with conduction gaps in PV encircling lesions, has been described. Moreover, the PV echo was induced only at the specific pacing CL. Atrial impulse-triggered PV echo has not been reported at the present moment. Bun and colleagues observed double PV response to a single PV stimulus within the electrically isolated PV1. In our patient, however, PV echo was not inducible after the LSPV was electrically isolated from the LA. Recently we reported sinus impulse-triggered echoes within superior vena cava (SVC) resulting in atrial bigeminy, although response of the SVC to programed atrial stimulation was not evaluated2. In conclusion, the atrial rate-specific repetitive PV response resulting in atrial premature beat is a newly observed phenomenon that may provide insights into the arrhythmogenesis of the incompletely ablated PV muscular sleeves.