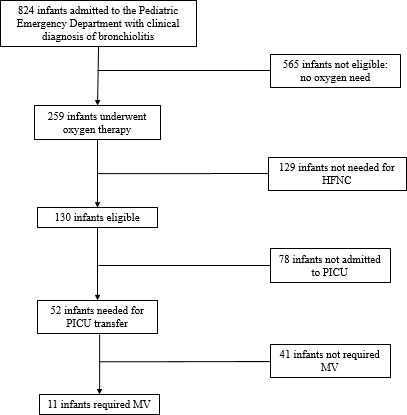
Introduction Acute bronchiolitis is the most common respiratory illness and the main cause of respiratory failure in infant. Effective therapy is not available. A relatively new, safe and promising method of non-invasive respiratory support is oxygen delivery by high-flow nasal cannula (HFNC), but several questions concerning HFNC clinical practice remain unanswered. Aim The main aim of our study is to analyse the clinical course of infants hospitalized for bronchiolitis who underwent HFNC in order to identify clinical, laboratory or radiological findings that can have an impact on HFNC failure, which is defined as requirement for mechanical ventilation (MV). Methods We conducted a retrospective data analysis of case records of 130 patients less than 12 months hospitalized for bronchiolitis who underwent HFNC and clinical epidemiological laboratory and radiological data were collected. Results Only 11 (8.5%) out 130 infants required invasive mechanical ventilation for clinical deterioration. Patients who needed to switch from HFNC to MV because of a progressive respiratory failure showed more frequently a complete upper lobe consolidation on CXR (90.9%) than infants exclusively supported by HFNC (14.9%). They were younger with a lower admission weight and they had a lower lymphocyte count than patients who underwent HFNC only. Discussion Our study suggests that a complete upper lobe consolidation in young infants is a significant risk factor for HFNC failure. Further studies are needed to understand if an early identification of consolidation following by an adequate follow-up and proper therapeutic strategies may reduce the number of children who require mechanical ventilation.