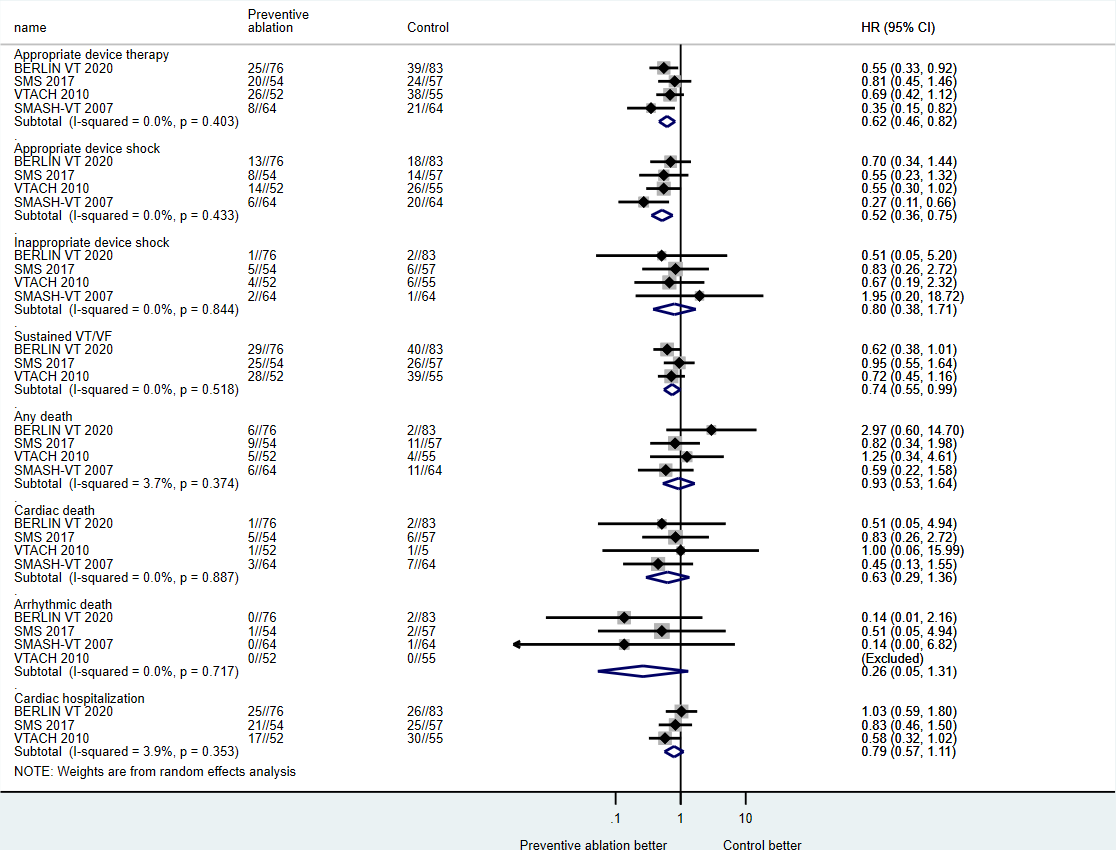
Introduction: In patients with post-infarct cardiomyopathy and ventricular arrhythmias (VT) necessitating implantable cardioverter defibrillators (ICD) are at risk of recurrent shocks with increased morbidity. Methods and Results: A comprehensive search of electronic databases for all randomized clinical trials that evaluated the role of catheter ablation as a preventive strategy at the time of secondary prevention ICD implantation was performed. Four trials were identified with a total of 505 patients (average age 66.4 ± 9.0 yr; 87.7% were male). Preventive ablation was associated with a significant reduction in appropriate device therapies (shocks and/or anti-tachycardia therapy) (hazard ratio [HR]=0.62; 95% confidence interval [CI]=0.46-0.82; p<0.01), sustained VT (HR=0.74; 95% CI=0.55-0.99; p=0.04) compared to control. There were no differences in inappropriate device shocks (HR=0.80; 95% CI=0.38-1.71), all-cause death (HR=0.93; 95% CI=0.53-1.64), cardiac death (HR=0.63; 95% CI=0.29-1.36), arrhythmic death (HR=0.26; 95% CI=0.05-1.31), or cardiac hospitalization (HR=0.79; 95% CI=0.57-1.11) between strategies. Preventive ablation was associated with improved SF-36 physical component (SMD=2.81; 95% CI-0.53-5.10; p=0.02), but not the mental component (SMD=1.30; 95% CI=-2.06-4.66). Conclusion: Among patients with post-infarct cardiomyopathy and VT, preventive catheter ablation at the time of ICD implantation is associated with a significant reduction of appropriate ICD therapy and sustained VT, and improvement in the physical component of quality-of-life, but no reduction in mortality.