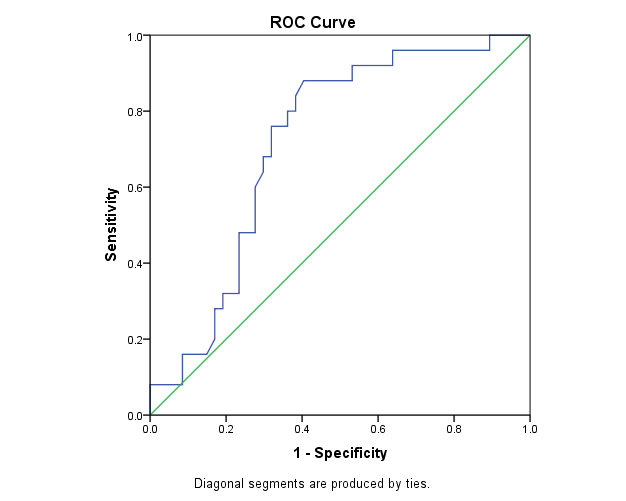
Background: Doppler echocardiographic parameters of the middle hepatic vein (MHV)in detecting PHTN. Methods: The study comprised 72 patients who were referred for right heart catheterization (RHC) to our department . All patients underwent conventional transthoracic echocardiography (TTE) the day after RHC and Doppler study of the MHV. Based on RHC and TTE results, Patients were divided in three groups 1: patients with PHTN without significant RV dysfunction (n=25), 2: patients with PHTN with significant RV dysfunction (n=22), 3: patients with normal PAP (n=25). Results: The analysis revealed a significant relationship between A velocity and PHTN among patients with significant RV dysfunction (p=0.033) and PHTN without significant RV dysfunction (p=0.020). At cut-off value of 39.5 cm/s, A velocity could detect PHTN in patient with significant RV dysfunction with sensitivity and specificity of 77.3% and 56.0%, respectively. At cut-off value of 38.5 cm/s, A velocity could detect PHTN without significant RV dysfunction with sensitivity and specificity of 76.0% and 51.0%, respectively. The ROC curve analysis was performed to assess the sensitivity of the hepatic venous systolic filling fraction in detecting normal SPAP in the study population. The area under curve was 0.718. Considering the cut-off value of 0.535 for the hepatic venous systolic filling fraction, the sensitivity and specificity of S/S+D for detecting normal SPAP were 80% and 64%, respectively . Discussion: Doppler echocardiographic parameters of the MHV could be helpful in detecting PHTN. A/S higher than 1 in PHTN was the main finding on HV Doppler assessment in PHT with and without significant RV dysfunction. HV systolic filling fraction more than 0.535 was a sensitive parameter in detecting normal PAP, therefore; HV systolic filling fraction can be used as a screening echocardiographic parameter in ruling out PHTN.