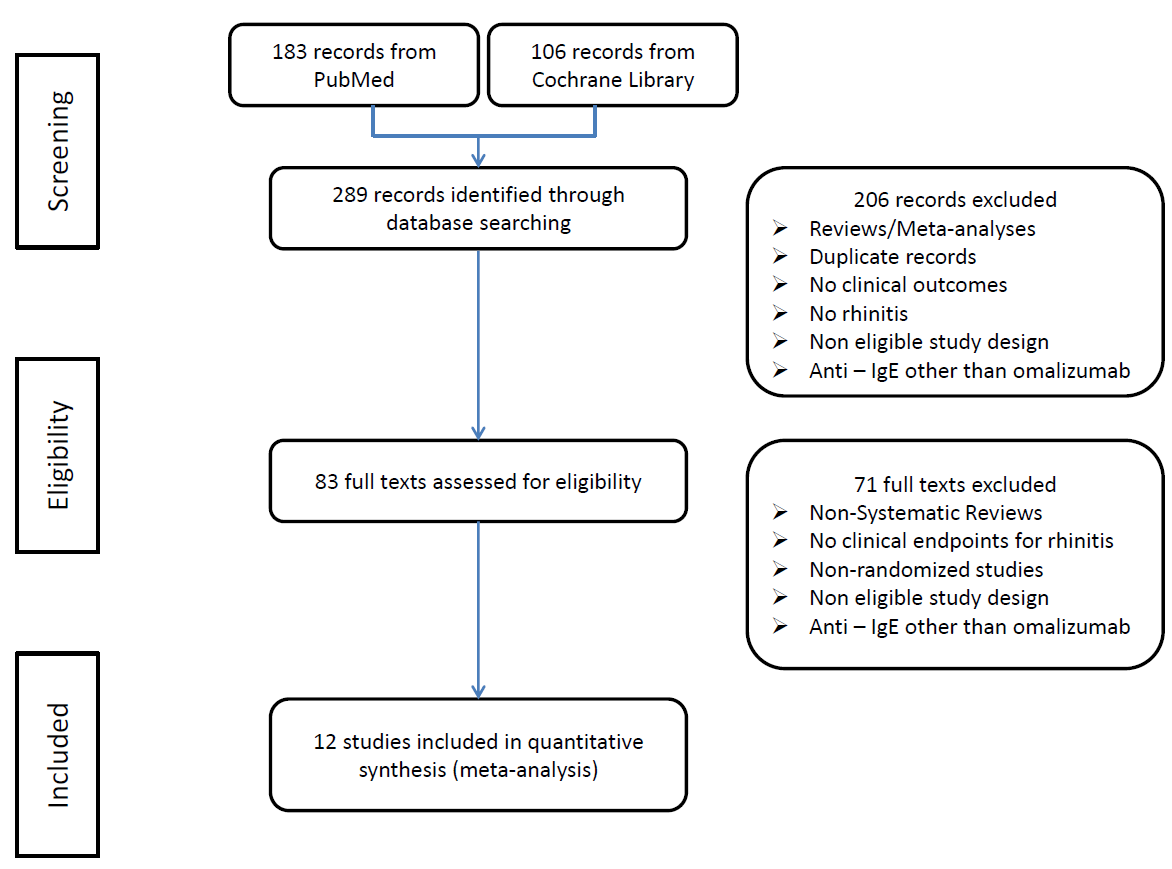
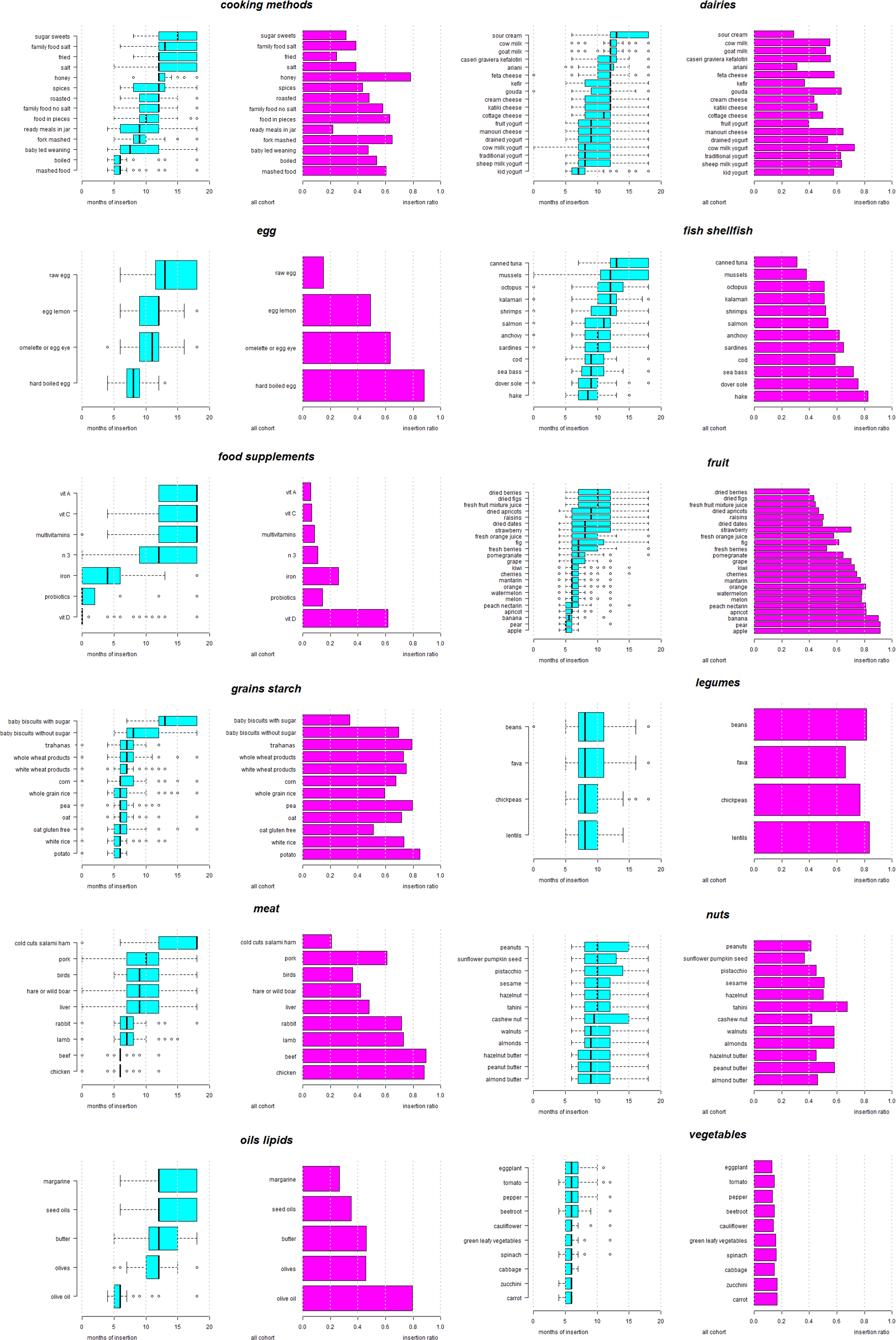
Background Recommendations have been issued on healthy complementary feeding (CF) strategies for infants, to reduce food allergy. This is a study of routine guidance provided by Greek pediatricians on the timing of CF for healthy infants and those at high risk for allergy. Methods Pediatricians in Greece completed an anonymous online questionnaire covering demographic information and recommended CF, specifically the foods, preparation methods, supplements, time interval between introduction of new foods for infants at low and high risk for allergy, and foods delayed in the case of high allergy risk. Results The respondents (n=233) recommended introducing: at 6 months, fruits, starchy non-gluten-grains, vegetables, olive oil and meat; at 7 months, gluten-rich grains; at 8 months, yogurt, hard-boiled egg and legumes; at 8.5 months, fish; at 9 months, nuts. A longer interval between new foods (≥ 4 days) was recommended, for low-risk infants, by male pediatricians (p=0.04), and for infants at high risk of allergy, by pediatricians with no subspecialty (p<0.001) and those practicing in a rural/semi-urban area (p=0.002). Pediatric practice of < 15 years was a predictor for earlier introduction of egg, seafood, gluten-rich grains, legumes and nuts for infants at high risk of allergy, and parenthood and male sex for egg and grains. Conclusions Greek pediatricians use a food introduction schedule for CF of infants, and, although not explicitly recommended in current guidelines, they delay introduction of common food allergens and suggest longer time intervals between introduction of new foods, especially for infants at high risk of allergy.