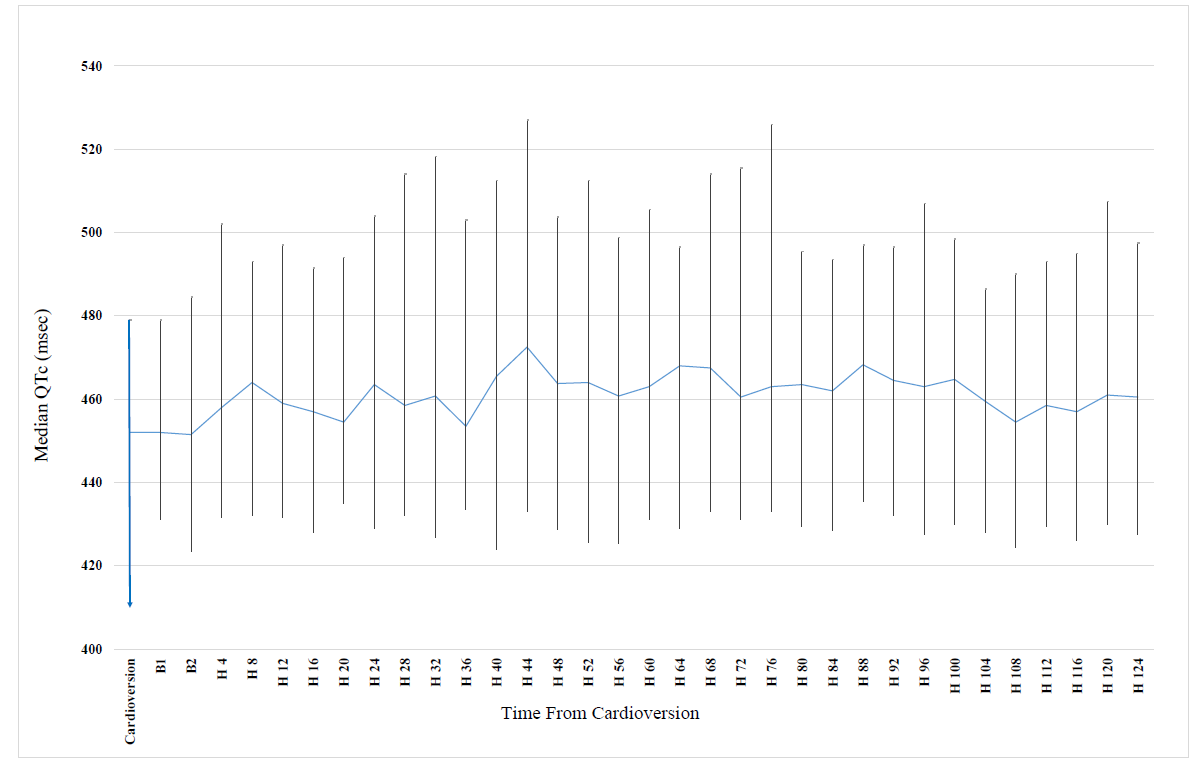
Introduction – We aimed to assess changes in QTc over time following cardioversion (CV) for persistent atrial fibrillation (AF), and to compare the benefit of using continuous Holter monitoring vs. conventional follow-up. Methods – The study population comprised 90 patients admitted to our center for elective CV due to persistent AF who were prospectively enrolled from July 2017 through August 2018. All patients underwent 7-day Holter started prior to CV. Baseline QTc was defined as median QTc during first hour post CV. The primary endpoint was QTc prolongation defined as QTc ≥500ms, or ≥10% increase (if baseline QTc was >480ms). Conventional monitoring was defined as an ECG recording 2-hours post CV. McNemar test was used for comparison. Results - Mean age was 67 ± 11 years and 61% were male. Median baseline QTc was 452msec (IQ range: 431-479 msec) as compared with a maximal median QTc of 474msec (IQ range: 433–527 msec; p<0.001 for the change in QTc from baseline). Peak median QTc occurred 44-hours post CV. The primary endpoint was met in 3 patients (3%) using conventional monitoring, compared with 39 new patients (43%) using Holter (p<0.001 for comparison). The Holter monitoring was superior to conventional monitoring in detecting clinically significant QTc prolongation (OR=13; p<0.001). Conclusion – CV of patients with persistent AF may be associated with increased transient risk of QTc prolongation. Peak median QTc occurs during end of second day following CV and prolonged ECG monitoring provides superior detection of significant QTc prolongation compared with conventional monitoring