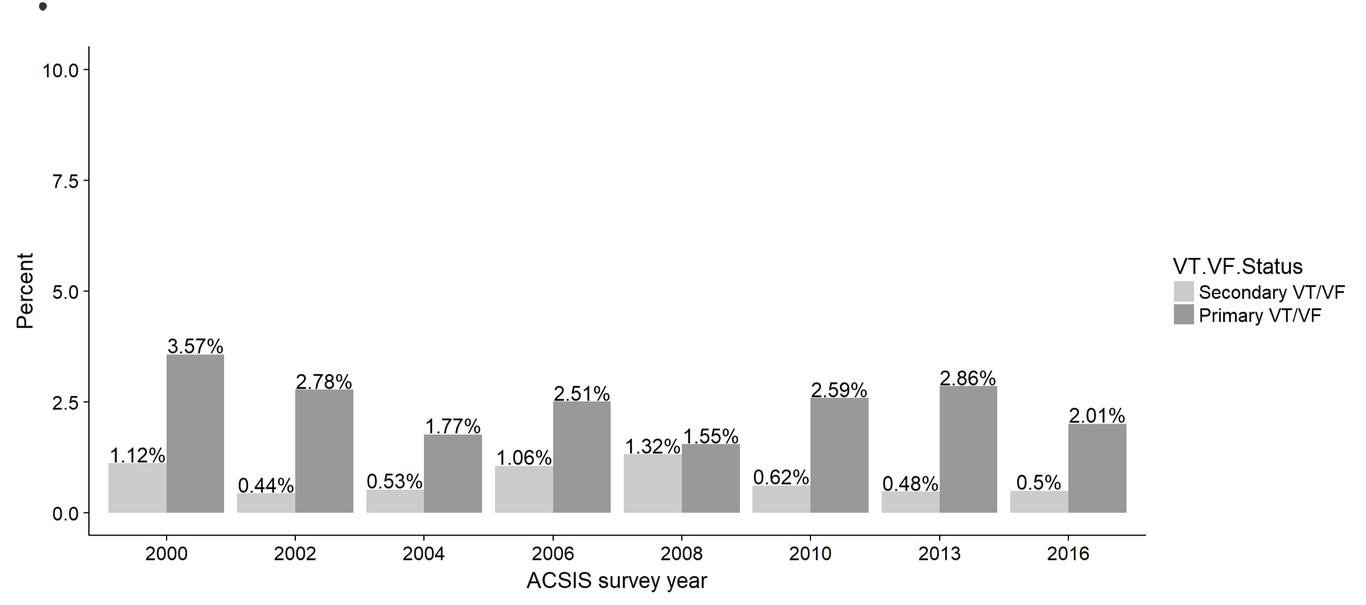
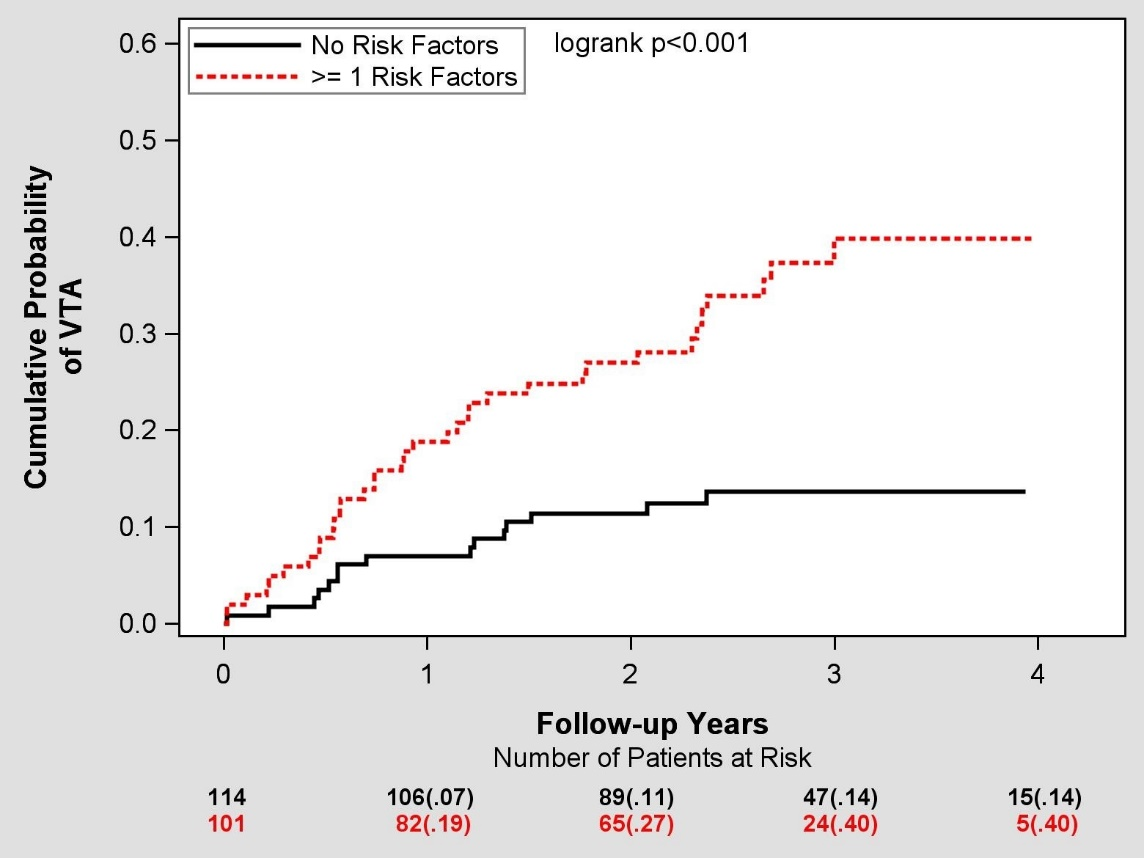
Objectives: To evaluate clinical characteristics and prognosis of patients presented with ventricular tachyarrhythmia (VTA) during the course of acute coronary syndrome (ACS) and to analyze it according to period of presentation. Background: VTA is an infrequent yet serious complication of ACS. There is limited data regarding the incidence and prognostic implications of VTA in the last decade as compared with the previous decade. Methods: We evaluated clinical characteristics, major adverse cardiovascular events, short and long- term mortality of patients hospitalized with ACS who were enrolled in the Acute Coronary Syndrome Israeli Survey (ACSIS) during the years 2000-2016. Patients were classified into three groups: no VTA, early VTA (≤48h of onset) and late VTA (>48h of onset). Data were analyzed according to decades of presentation (current decade vs. previous decade). Results: The study population comprised 15,200 patients. VTA occurred in 487 (3.2%) of patients. Early VTA presented in 373/487 (77%) patients and late VTA in 114/487 (23%) patients. VTA’s, occurring in ACS patients were associated with increased risk of in-hospital, 30-days, 1-year and 5-year mortality rates during both early and late periods in compared with no VTA. Moreover, late VTA was associated with the highest mortality rate with up to 65% in 5-year follow up (p<0.001). Nevertheless, late VTA was associated with lower mortality rate in the current decade (2008-2016) compared with last decade (2000-2006). Conclusions: Any VTA following ACS was associated with high short and long-term mortality rate. However, over the past decade there has been a significant improvement in survival rates, especially in patients with late VTA. This may be attributed to early and invasive reperfusion therapy, implantable cardioverter defibrillator implantation and better medical treatment.