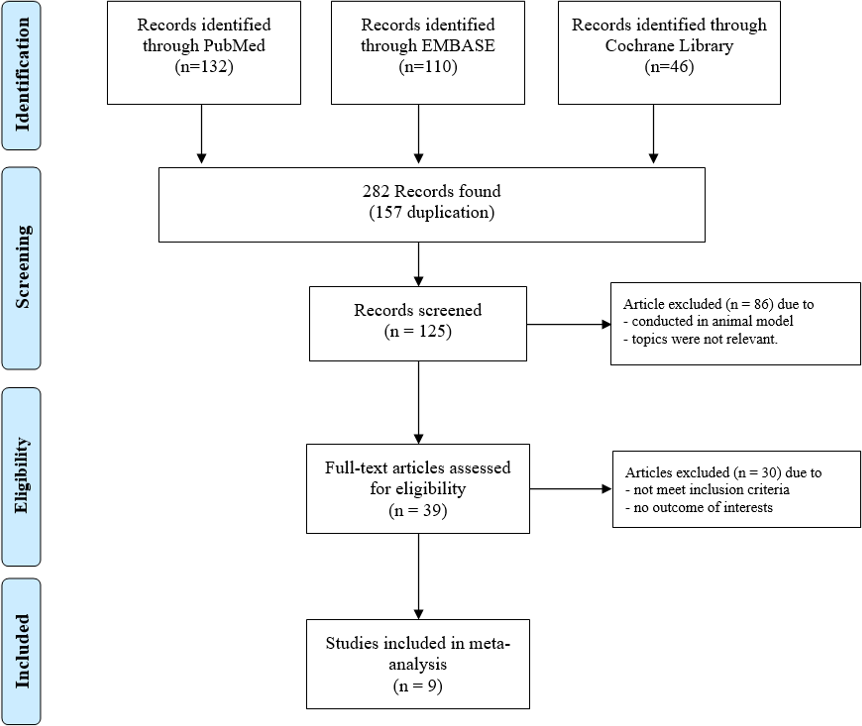
Background: Multiple strategies have advocation for power titration and catheter movement during atrial fibrillation (AF) ablation. Comparative favoring evidence regarding the efficacy, logistics, and safety of a higher power, shorter duration (HPSD) ablation strategy compared to a lower power, longer duration (LPLD) ablation strategy is insubstantial. We performed a meta-analysis to compare arrhythmia-free survival, procedure times, and complication rates between the two strategies. Methods: We searched MEDLINE, EMBASE and Cochrane Library from inception to April 2020. We included studies comparing patients underwent HPSD and LPLD strategies for AF ablation and reporting either of the following outcomes: freedom from atrial tachyarrhythmia (AT) including AF and atrial flutter, procedure time, or periprocedural complications. We combined data using the random-effects model to calculate odds ratio (OR) and weight mean difference (WMD) with 95% confidence interval (CI). Results: Nine studies from 2006-2020 involving 2,282 patients were included (1,369 patients underwent HPSD strategy and 853 patients underwent LPLD strategy). HPSD strategy was not associated with an increased freedom from AT at 12-month follow-up (OR= 1.41, 95%CI:0.90-2.21). There was a significant reduction in the HPSD group for total procedure (WMD=49.60, 95%CI:29.76-69.44) and ablation (WMD=17.92, 95%CI:13.63-22.22) times, but not for fluoroscopy time (WMD=1.15, 95%CI:-0.67-2.97). HPSD was not associated with a reduction in esophageal ulcer/atrioesophageal fistula (OR=0.35, 95%CI:0.12-1.06) or pericardial effusion/cardiac tamponade rates (OR=0.96, 95%CI:0.24-3.79). Conclusions: When compared to a LPLD strategy, HPSD strategy does not improve recurrent AT nor reduce periprocedural complication risks. However, a HPSD strategy can significantly reduce total procedure and ablation times.