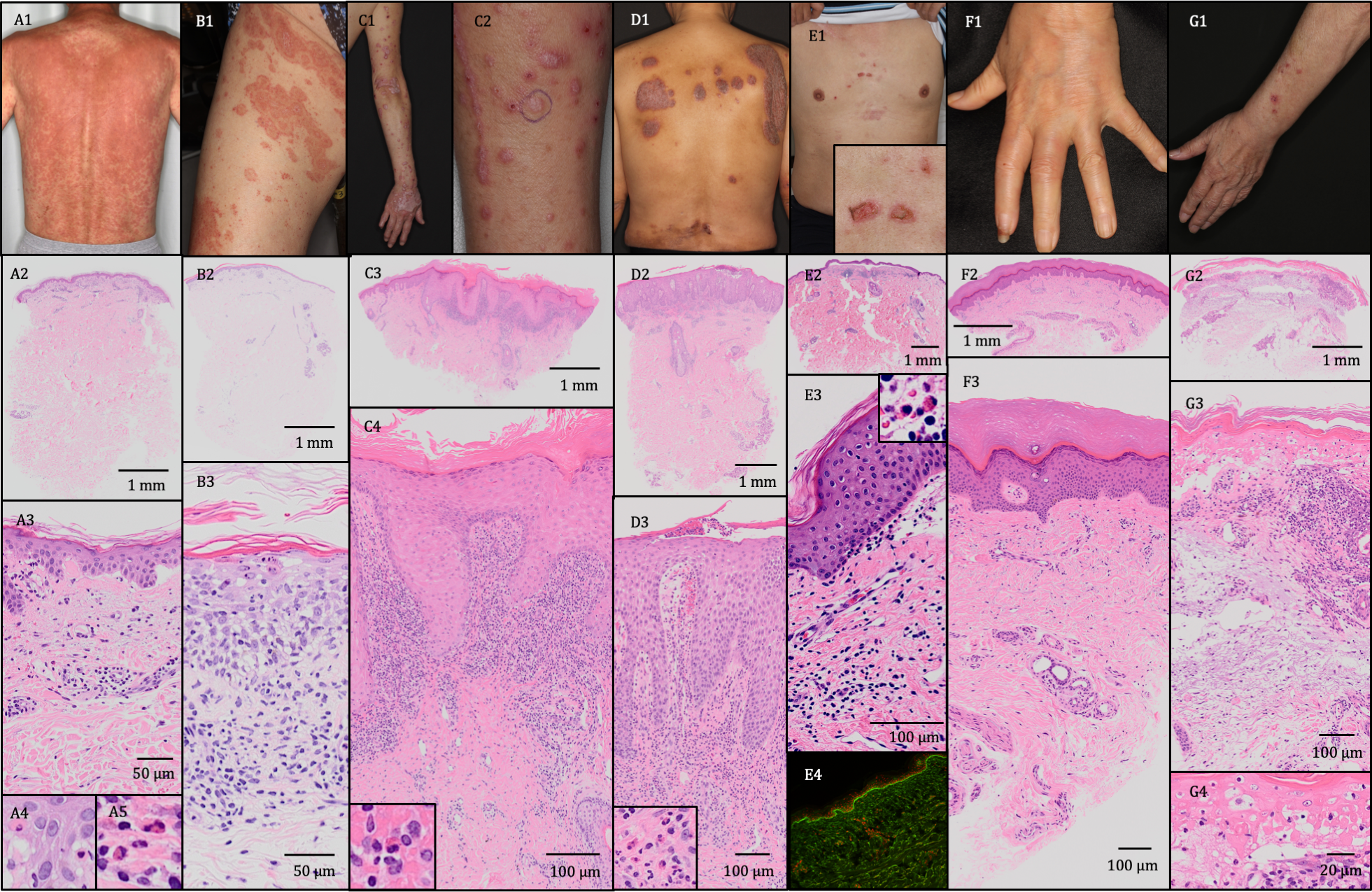
Background: Immune checkpoint inhibitors (ICIs) cause a variety of inflammatory eruptions. A better understanding of the rash types, histopathological findings, severity, and clinical courses is necessary for appropriate managements of these eruptions. Only a few reports reviewed ICI-induced inflammatory eruptions with detailed histopathological findings. Methods: In this study, we retrospectively reviewed 42 patients who were histopathologically diagnosed with cutaneous immune-related adverse events (irAEs) following ICI therapy between 2014 and 2020 at the Department of Dermatology of Kyushu University Hospital. Results: Of the 42 patients (24 males, 18 females), maculopapular rash (33/42, 78.6%), erythema multiforme (2/42, 4.8%), lichenoid reaction (3/42, 7.1%), psoriasiform reaction (1/42, 2.4%), bullous pemphigoid (1/42, 2.4%), scleroderma-like reaction (1/42, 2.4%), and Stevens-Johnson syndrome (1/42, 2.4%) were observed. The clinical and histopathological findings of these eruptions were equivalent to typical cases of common drug eruptions. The onset of maculopapular rash was relatively early (more than half of events occurred within 1 month), whereas lichenoid reactions and autoimmune diseases occurred relatively late (4–8 m¬¬onths). With appropriate treatment and/or interruption of ICIs, most rashes were improved (40/42, 95.2%). Conclusions: The ICI-induced inflammatory eruptions shared similar clinical and histopathological features with classical inflammatory eruptions, but a variety of inflammatory eruptions may occur with different degrees of severity. Dermatologists play an important role in providing specialized care for cutaneous immune-related adverse events.