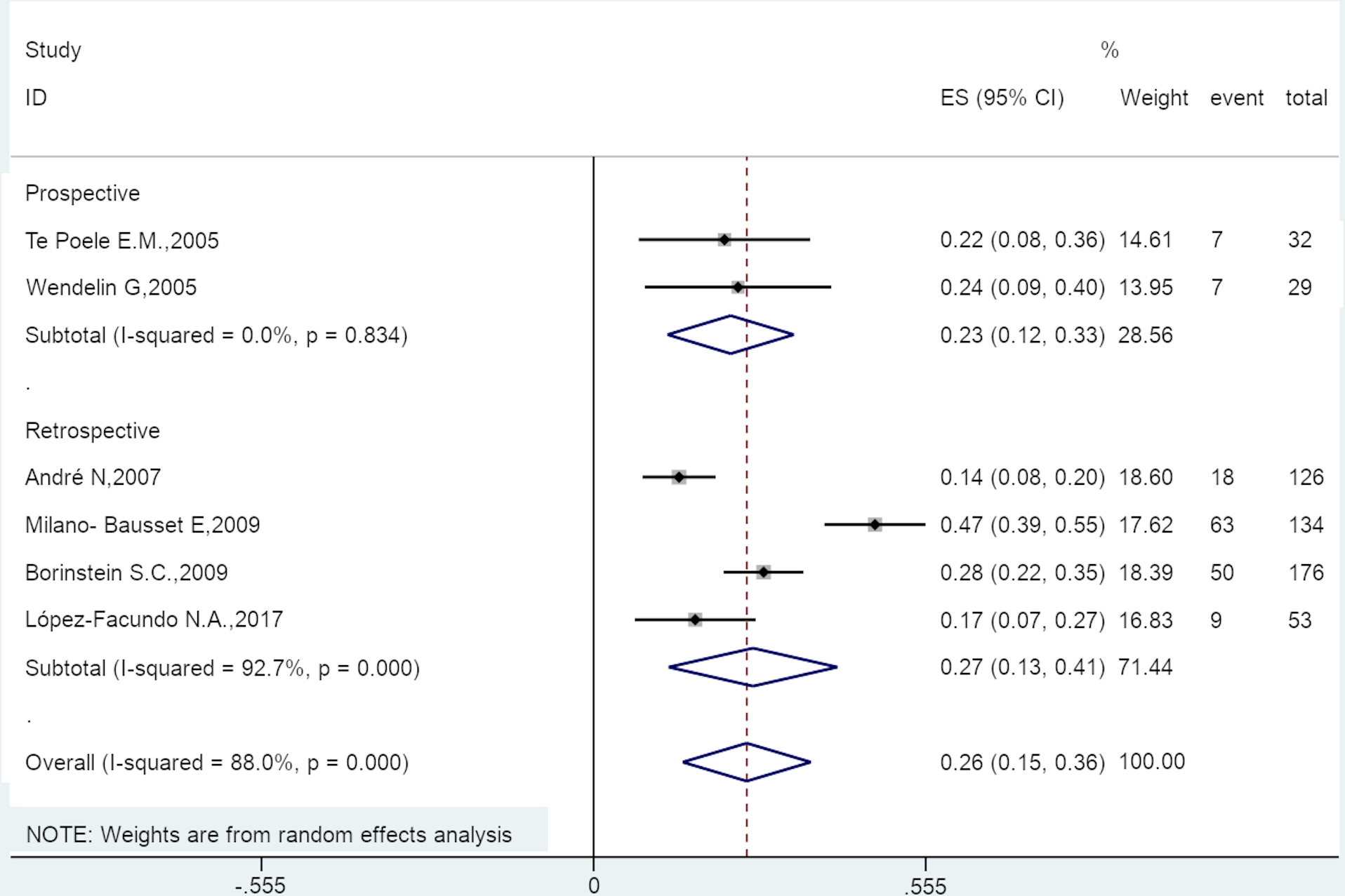
Background: Granulocyte colony-stimulating factors (G-CSF) can be used as prophylaxis for febrile neutropenia (FN) in adults. There is no meta-analysis about the effects of pegfilgrastim on the occurrence of FN in pediatric/adolescent cancer patients. Purpose: To determine the effect of pegfilgrastim on FN in pediatric and adolescent cancer patients. Methods: PubMed, Embase, and the Cochrane library were searched for studies published prior to April 7, 2020. The outcome was the occurrence of FN. For analyses showing high heterogeneity (I2>50% and Q-test P<0.10), the random-effect model was used; otherwise, the fixed-effect model was used. Results: Eight studies were included, comprising 167 patients and 550 courses of treatment. Pegfilgrastim decreased the rate of FN compared with controls (ES=0.26, 95%CI: 0.15-0.36, P<0.001); this was observed in prospective and retrospective studies. There was no difference between pegfilgrastim and filgrastim for the rate of FN in children receiving chemotherapy (OR=0.68, 95%CI: 0.20-2.23, P=0.520). Pegfilgrastim decreased the rate of grade 4 FN compared with controls (ES=0.40, 95%CI: 0.16-0.63, P=0.017); this was observed when analyzing the courses of treatment, but not the patients. Pegfilgrastim had no impact on treatment delays due to FN (ES=0.05, 95%CI: -0.00-0.10, P=0.061). Pegfilgrastim decreased the rate of severe neutropenia compared with controls (ES=0.39, 95%CI: 0.04-0.74, P=0.031). Conclusion: Compared with the control, pegfilgrastim significantly decreases the occurrence of FN, grade 4 FN, and severe neutropenia in pediatric patients receiving chemotherapy. Pegfilgrastim had no impact on treatment delays due to FN.