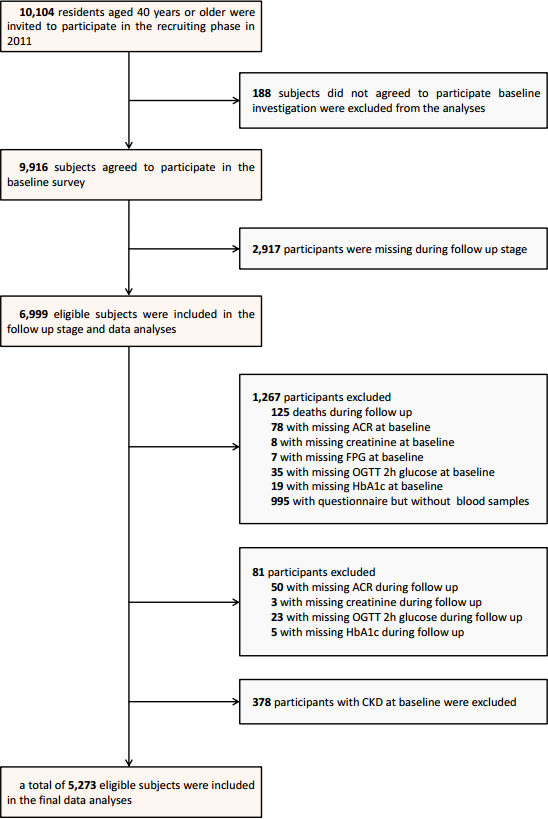
Background Chronic kidney disease (CKD) has become a major global health issue, and abnormalities of glucose metabolism are a risk factor responsible for development of CKD. We aimed to investigate associations between glucose metabolism indices and CKD in a Chinese population, and determine which index is superior for predicting incident CKD. Methods This community-based population study included 5232 subjects aged ≥40 years without baseline CKD. CKD was defined as an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 or urinary albumin-to-creatinine ration (UACR) ≥30 mg/g. We examined the associations of glucose metabolism indices, including fasting plasma glucose (FPG), 2-hour (2h) oral glucose tolerance test (OGTT), haemoglobin A1c (HbA1c), fasting insulin level, homeostasis model assessment of insulin resistance (HOMA-IR), and HOMA-β and the development of CKD. Results With an average follow-up of 3.6 years, 6.4% of the subjects developed CKD. Pearson’s correlation analysis revealed that FPG, HbA1c, fasting insulin, and HOMA-IR were all significantly correlated with UACR and eGFR. The association persisted in multivariate linear regression analysis adjusted for age and sex. Compared with other glucose indices, HOMA-IR exhibited the strongest associations with CKD in COX multivariate regression analysis (HR = 1.17, 95% CI: 1.04-1.31). Conclusion HOMA-IR is superior to other routine indices of glucose metabolism for predicting the development of CKD in middle-aged Chinese persons. Screening with HOMA-IR may help prevent the development of CKD in the general population.