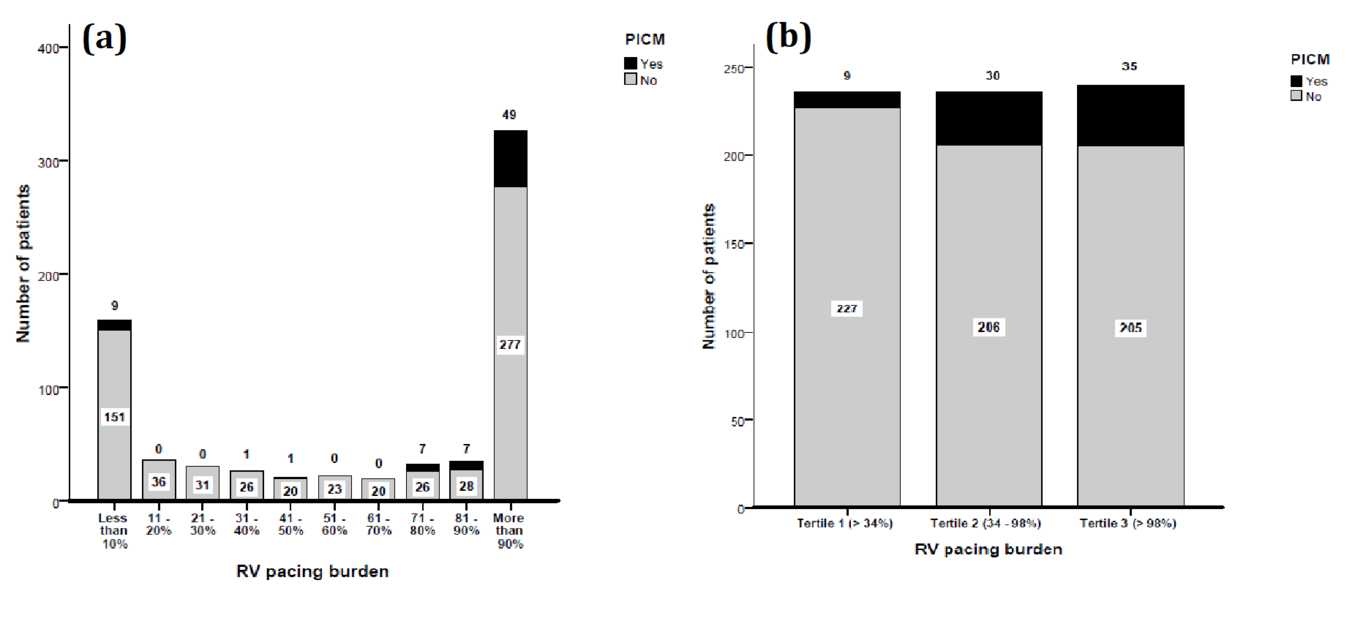
Introduction: Knowledge of factors causing pacing-induced cardiomyopathy (PICM) is incomplete. We sought to estimate the incidence and predisposing factors for PICM in South Asian population and evaluate if the risk they portend adds up. Methods: Consecutive patients with preserved LVEF undergoing pacemaker (PM) implantation between 2012 and 2018 were analysed. Results: A total of 749 patients (68.4% male; mean age 59.2 ± 14.08 years) were included in the analysis. PICM developed in 74 (9.9 %) patients over a median follow up of 2.2 years (IQR 1.1-3.2). Pre-implant LVEF, paced QRS duration and RV pacing burden were independent predictors of PICM. Using 90% specificity cut-off values for LVEF and paced QRS, and the value separating lowest tertile of RV pacing from the higher tertiles, three risk factors were identified: (i) baseline LVEF < 55%, (ii) paced QRS duration > 160 msec, and (iii) RV pacing burden > 33%. Patients with two or more risk factors were at the highest risk (OR 11.62, 95% CI 4.62 - 29.21, p-value < 0.001) for developing PICM while those with one risk factor had an intermediate risk (OR 3.89, 95% CI 1.62 - 9.34, p-value 0.002) when compared to those without any risk factors. Conclusion: Low-normal baseline LVEF, wider paced QRS and higher RV pacing burden independently predicted the development of PICM. The presence of ≥2 factors increased the odds of PICM, twelve-fold. Striving to get a narrower paced QRS, the only modifiable of the three risk factors, will help mitigate the development of PICM.