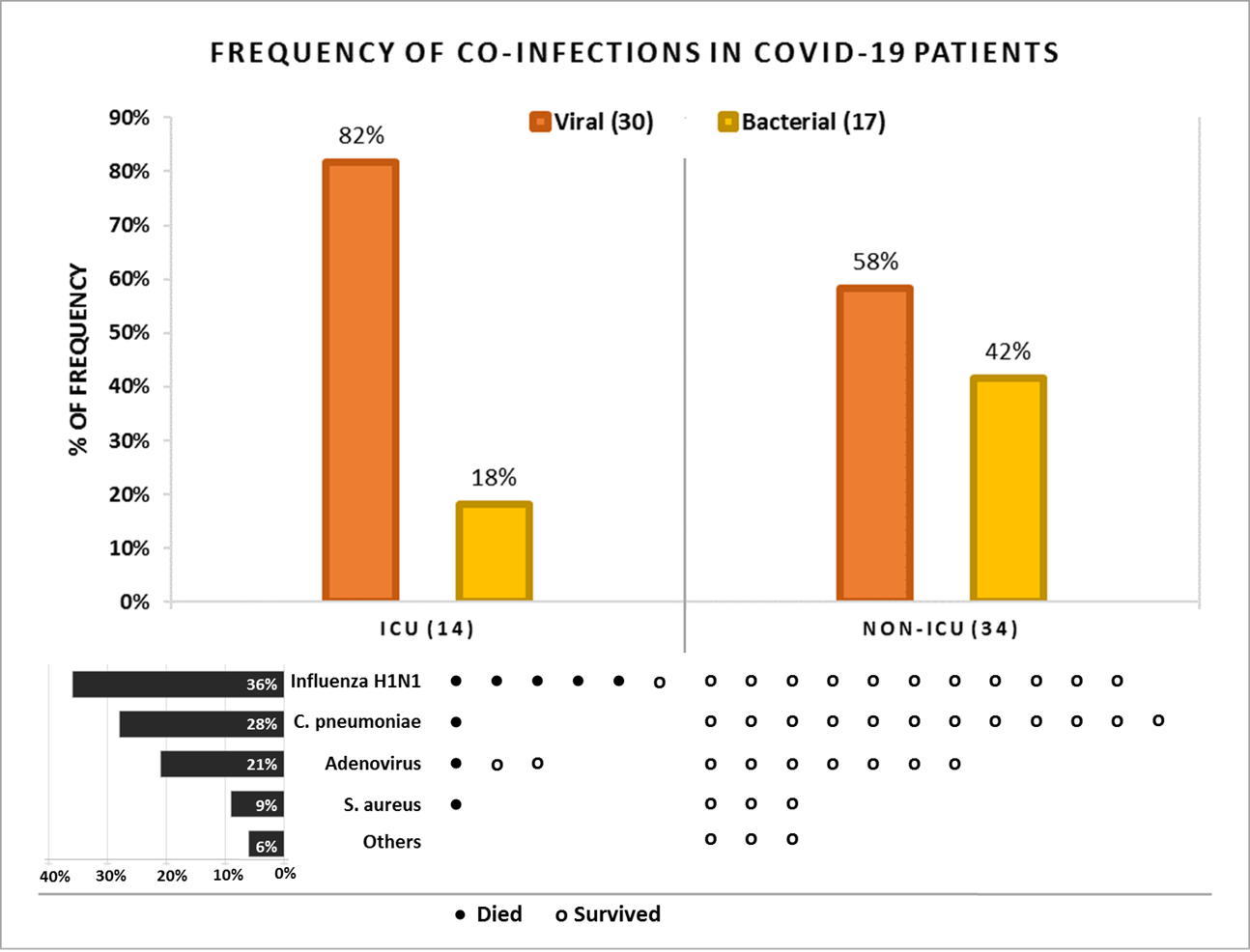
Background In COVID-19 patients, undetected co-infections may have severe clinical implications associated with increased hospitalization, varied treatment approaches and mortality. Therefore, we investigated the implications of viral and bacterial co-infection on COVID-19 clinical outcomes. Methods Nasopharyngeal samples were obtained from 48 COVID-19 patients (29% ICU and 71% non-ICU) and screened for the presence of 24 respiratory pathogens using six multiplex PCR panels. Results We found evidence of co-infection in 34 COVID-19 patients (71%). Influenza A H1N1 (n=17), Chlamydia pneumoniae (n=13) and human adenovirus (n=10) were the most commonly detected pathogens. Viral co-infection was associated with increased ICU admission (r=0.1) and higher mortality (OR 1.78, CI=0.38-8.28) compared to bacterial co-infections (OR 0.44, CI=0.08-2.45). Two thirds of COVID-19 critically ill patients who died, had a co-infection; and Influenza A H1N1 was the only pathogen for which a direct relationship with mortality was seen (r=0.2). Amongst comorbidities, co-infection in patients with diabetes was associated with a significantly higher mortality (p=0.02). We also found that Troponin T was strongly related (p=0.001) with ICU admission and could be used as a predictor of COVID-19 severity. Conclusions The similarity in clinical presentation for both COVID-19 and Influenza makes it difficult to assess their impact on ICU admission and mortality. Our study highlights the importance of screening for co-infecting viruses in COVID-19 patients, given the high prevalence of Influenza viruses. The detection of co-infections in COVID-19 cases shows the importance of flu vaccination and warrants its increased coverage to reduce the hospitalization and associated mortality.