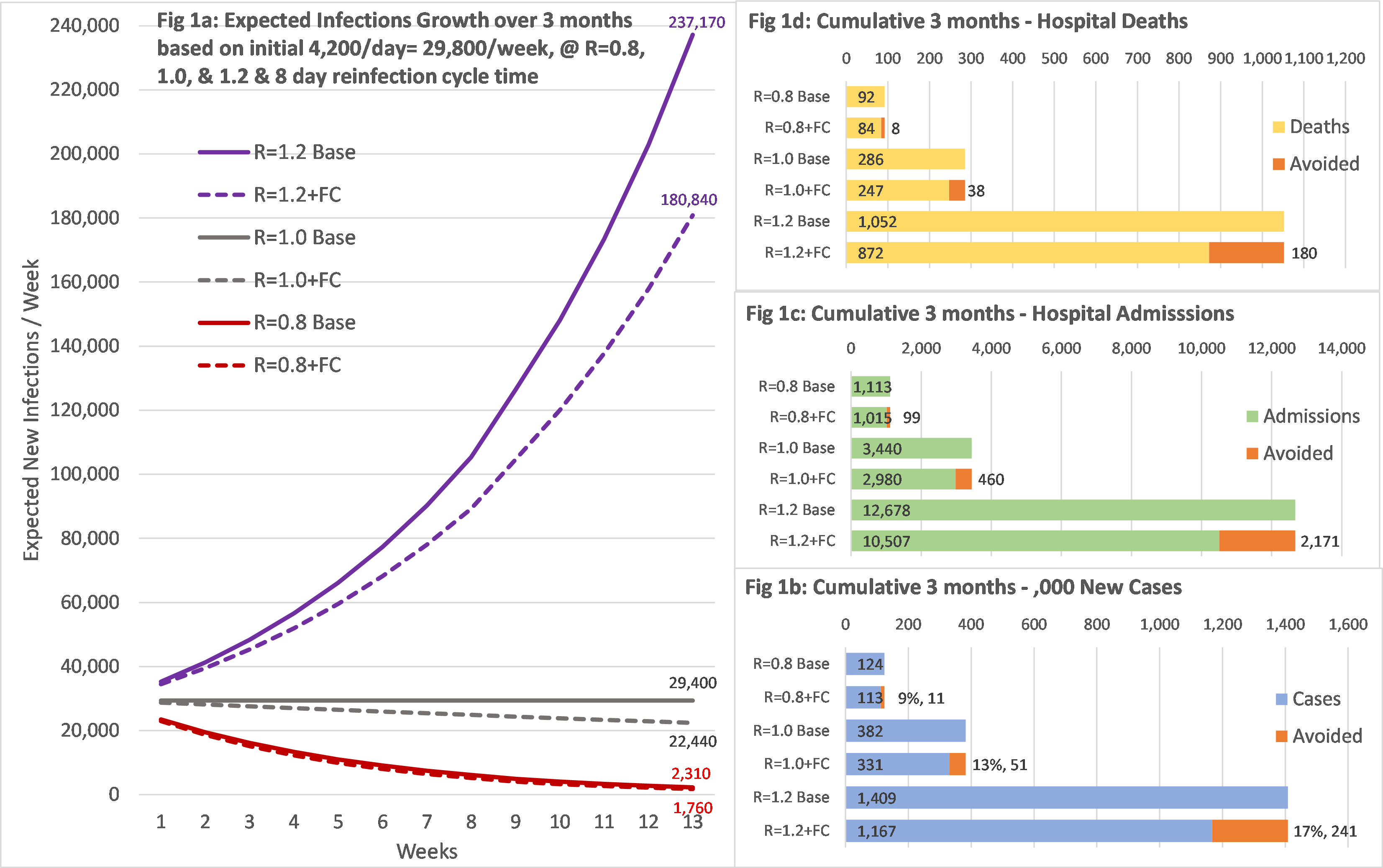
Introduction The rapid spread of the pandemic caused by the severe acute respiratory syndrome coronavirus 2(SARS-CoV-2)(COVID-19) virus resulted in governments around the world instigating a range of measures, including mandating the wearing of face coverings on public transport/in retail outlets. Methods We developed a sequential assessment of risk reduction provided by face coverings using a step-by-step approach. The United Kingdom Office of National Statistics(ONS) Population Survey data was utilised to determine the baseline total number of community-derived infections. These were linked to reported hospital admissions/hospital deaths to create case admission risk ratio/admission-related fatality rate. Results Overall, we show that only 7.3% of all community-based infection risk associates with public transport/retail outlets. The reported weekly community infection rate was 29,400 new cases at the start (24th July). The rate of growth in hospital admissions and deaths for England was around -15%/week, suggesting the infection rate, R, in the most vulnerable populations was just above 0.8. In this situation, average infections over the evaluated 13week follow-up period was 9,517/week. With face covering of 40% effectiveness, this reduced average infections by 844/week, hospital admissions by 8/week and deaths by 0.6/week; a fall of 9% over the period total. If, however, the R-value rises to 1.0, then average community infections would stay at 29,400/week and face coverings could reduce average weekly infections by 3,930, hospital admissions by 36 and deaths by 2.9/week; a 13% reduction. These reductions should be seen in the context of 102,000/week all-cause hospital emergency admissions in England and 8,900 reported deaths in the week ending 7thAugust 2020. Conclusion We have illustrated that the policy on mandation of face coverings in retail outlets/on public transport may have limited value in reducing hospital admissions/deaths. Impact appears small compared to all other sources of risk, thereby raising questions regarding effectiveness of the policy.