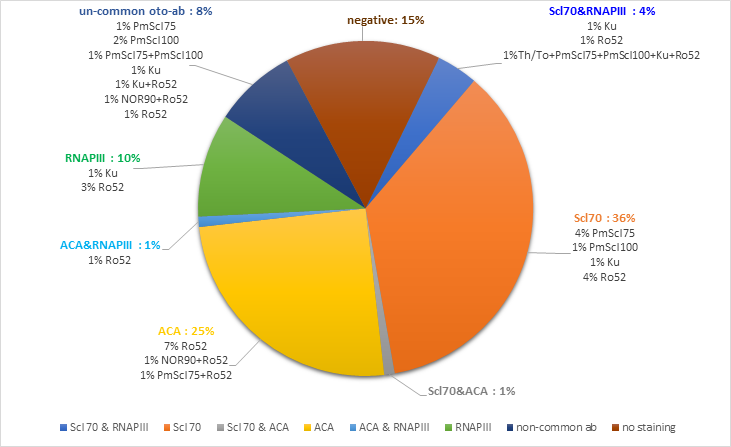
Background/aim: To investigate the frequency and clinical relevance of an extended autoantibody (ab) profile in patients with SSc. Materials and Methods: In this cross-sectional study, serum from 100 consecutive patients was subjected to indirect immunofluorescence (HEp-20-10/primate liver mosaic) and Systemic Sclerosis Profile by EUROIMMUN (Lübeck, Germany) to evaluate ANA and autoantibodies against 13 different autoantibodies in patients with SSc less than three years. Results: 93 of 100 patients were positive for ANA by indirect immunofluorescence (IIF). The prevalence of Anti-Scl70 ab was 41%, anti-centromere (ACA) 27%, and anti-RNA polymerase (RNAPIII) 15%. Scl70 was more associated with diffuse subtype (p<0.001), ILD (p<0.001), and high mRSS (p=0.002); ACA with limited disease (p<0.001), less ILD (p<0.001), overlap (p=0.017) and low mRSS (p=0.024); RNAPIII with diffuse disease (p=0.027), ILD (p=0.016) and high mRSS (p=0.001). Fifty-three patients showed single positivity (26 anti-Scl70, 16 ACA, 6 anti-RNAPIII, 1 anti-Ku ab, 1 anti-PM/Scl100, 2 anti-PM/Scl75, 1 anti-Ro52), whereas 32 patients had multiple auto-antibody positivities. Among common SSc-specific autoantibodies, Scl70 and RNAPIII showed the highest co-occurrence (n=4). One patient was simultaneously positive for anti-RNAPIII ab and ACA, and one was positive for ACA and Scl70. The clinical features were not statistically different between single and multiple autoantibody-positivity for common SSc-specific autoantibodies (ACA, Scl70, and RNAP III), except for digital ulcer in multi-antibody positive ACA group (p=0.019). Conclusion: Based on our results, co-expression of auto-antibodies is not uncommon in SSc patients. Although SSc-specific auto-antibodies generally show known clinical features, the clinical presentation of the co-expression in specific and non-specific auto-antibody positivity continues to be important.