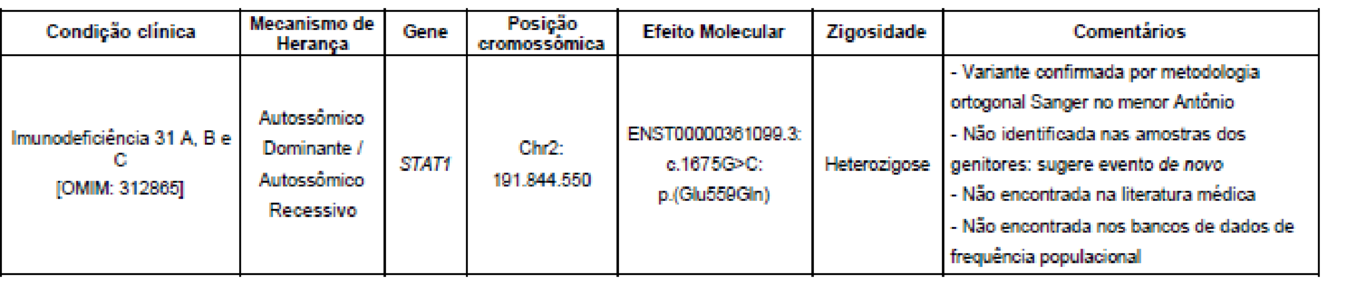
Would STAT1 GOF prevent severe forms of COVID-19?To the Editor:As the world faces the current SARS-CoV-2 pandemic, the scientific community struggles to answer questions about the disease that have not been fully clarified yet. It is well known that individuals with certain chronic diseases are at higher risk of having worse prognosis when infected with this virus. Although the risk of a severe disease is still a matter of conjecture in subjects with Inborn errors of Immunity (IEI), these patients may present more COVID-19 complications than the general population, either by community acquired or nosocomial infection1.In our immunology referral clinic at the Federal University of São Paulo (UNIFESP), so far, 16 IEI patients have been diagnosed with COVID-19, with a large spectrum of presentation, ranging from mild disease to severe acute respiratory syndrome and death. One of them, however, had a favorable outcome, with no complications, after being infected with the SARS-CoV-2, despite his several serious comorbidities.We report the case of an 11- year -old boy, diagnosed with Type 1 Diabetes Mellitus at the age of 3 years. At that time, he presented persistent watery diarrhea, 3 to 4 episodes a day. One year later, productive cough, persistent fever, conjunctival hyperemia and generalized lymph node enlargement emerged. Histoplasma sp. was isolated in ocular secretion. Acute Disseminated Histoplasmosis (pulmonary, ocular and ganglionic) was diagnosed and he received Itraconazole for one year.In 2018, at the age of 9 years, we started to follow him at our immunology clinic. He received all vaccines for his age with no adverse events. The family reported recurrent skin infections, repeated pneumonia, mucocutaneous and esophageal candidiasis, and arthralgia. He presented hepatomegaly and failure to thrive. The main diagnostic hypothesis was a disease of immune dysregulation. Screening for inborn errors of immunity and inflammatory lab tests were performed. White blood cell count, immunophenotyping and lymphocyte proliferation, serum immunoglobulins and dihydrorodamine (DHR) assay were in normal range. HIV serologies were negative. Whole exome sequencing was performed and the variant c.1675G> C (de novo variant) appeared in the STAT1 gene (Figure 1)3, in heterozygosis. To date, no data on this genetic variant has been published. This new finding is probably considered pathogenic and, due to the patient’s clinical characteristics, STAT1-GOF is very likely to be the diagnosis of our boy.