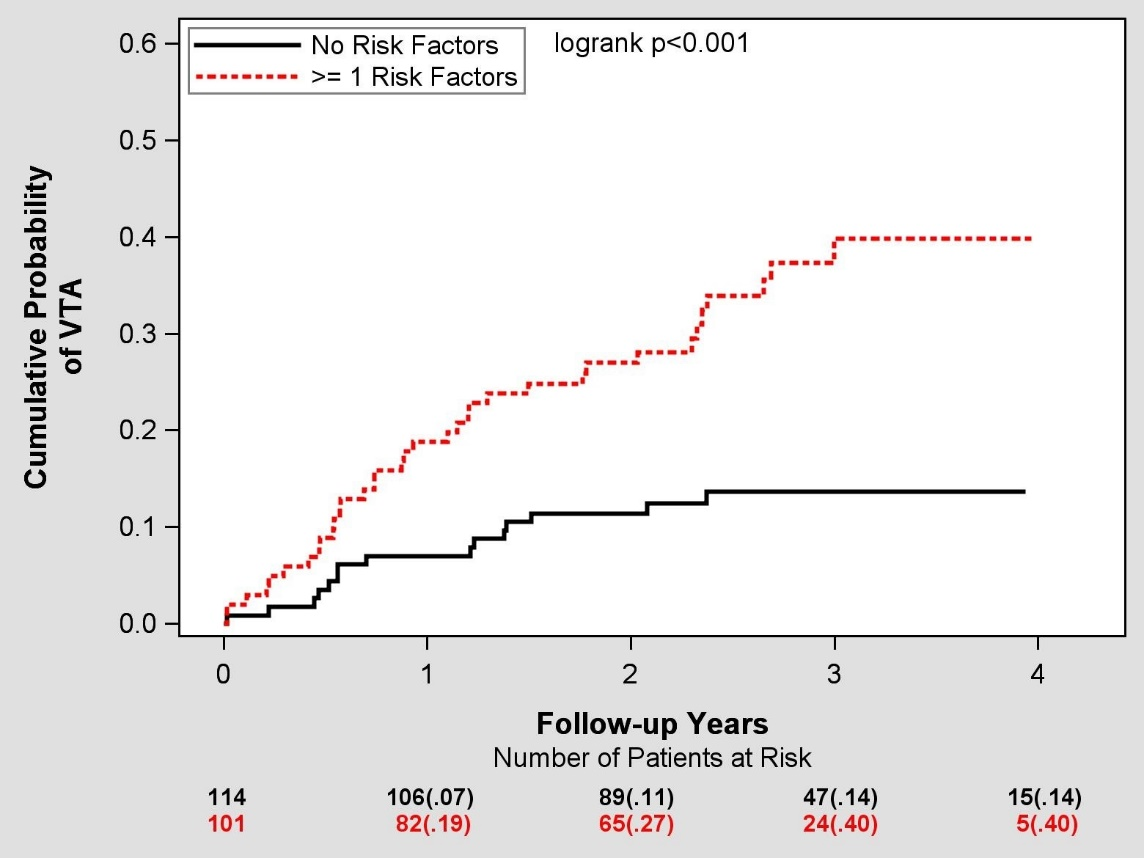
Introduction: Cardiac resynchronization therapy (CRT) may be proarrhtyhmic in patients with non-left bundle branch block (non-LBBB). We hypothesized that combined assessment of risk factors (RF) for ventricular tachyarrhythmias (VTA) can be used to stratify non-LBBB patients for CRT implantation. Methods: The study comprised 412 non-LBBB patients from MADIT-CRT randomized to CRT-D (n=215) vs. ICD-only (n=197). Best-subset regression analysis was performed to identify RF associated with increased VTA-risk in CRT-D patients without LBBB. The primary endpoint was first occurrence of sustained VTA during follow-up. Secondary endpoints included VTA/death, and appropriate shock. Results: Four RFs were associated with increased VTA risk: Blood Urea Nitrogen >25mg/dl, ejection-fraction <20%, prior non-sustained VT, and female gender. Among CRT-D patients, 114 (53%) had no RF, while 101 (47%) had ≥ 1 RF. The 4-year cumulative probability of VTA was higher among those with ≥ 1 RF compared with those without RF (40% vs. 14%, p<0.001). Multivariate analysis showed that in patients without RF, treatment with CRT-D was associated with a 61% reduction in VTA compared with ICD-only therapy (p=0.002), whereas among patients with ≥ 1 RF treatment with CRT-D was associated with a corresponding 73% (p=0.025) risk-increase. Consistent results were observed when the secondary endpoints of VTA/death and appropriate ICD shocks were assessed. Conclusion: Combined assessment of factors associated with increased risk for VTA can be used for improved selection of non-LBBB patients for CRT-D.