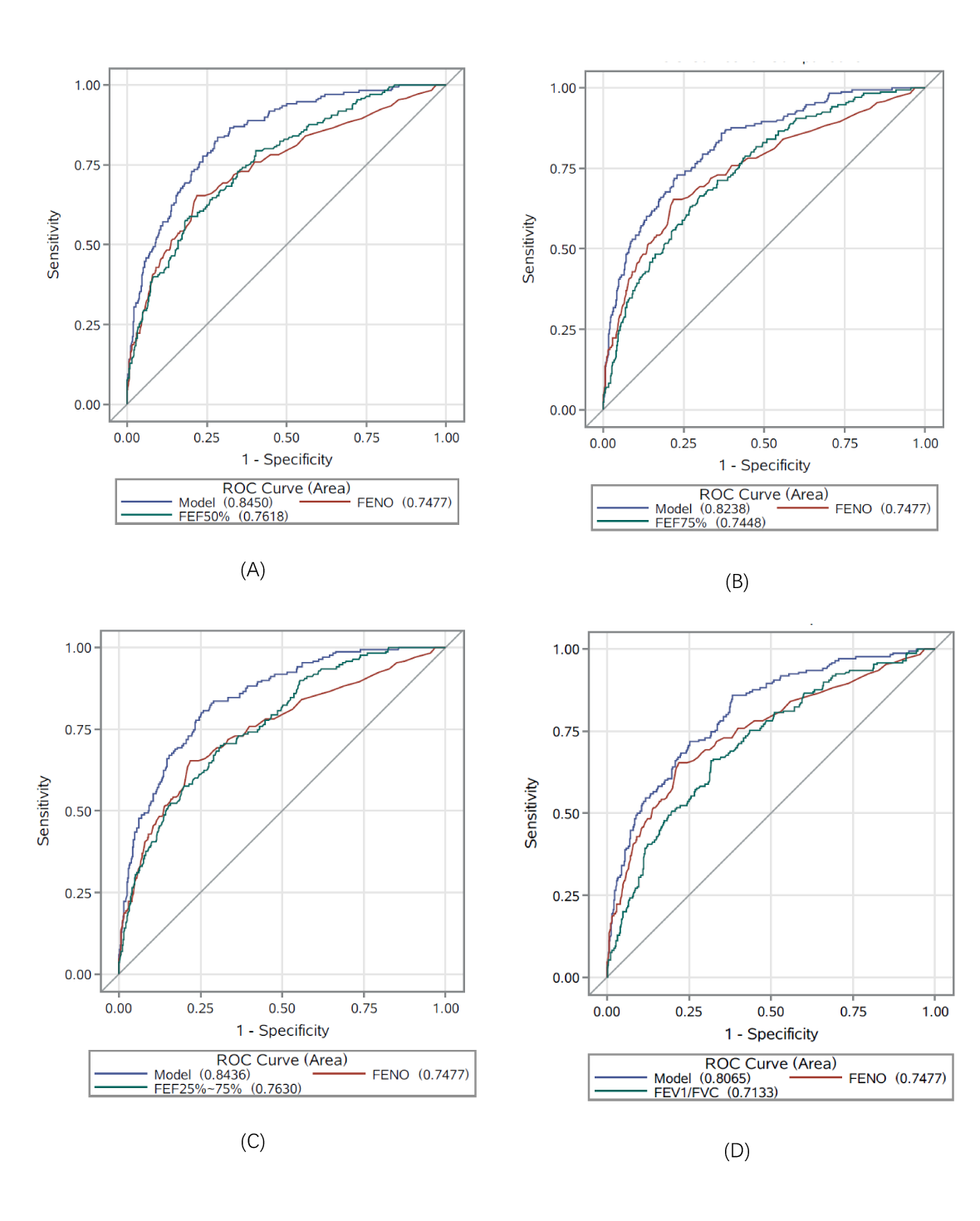
Background: Patients with variable symptoms suggestive of asthma but with normal forced expiratory volume in 1 second (FEV1) often fail to be diagnosed without a bronchial provocation test, but the test is expensive, time-consuming, risky and not readily available in all clinical settings. Methods: A cross-sectional study was performed in 692 patients with FEV1≥80% predicted; normal neutrophils and chest high-resolution computed tomography; and recurrent dyspnea, cough, wheeze, and chest tightness. Results: Compared with subjects negative for BHR (n=522), subjects positive for BHR (n=170) showed increased FENO values, EOS, and R5-R20; decreased FEV1, FEV1/Forced vital capacity (FVC), and forced expiratory flow (FEFs) (P≤.001 for all). Small-airway dysfunction was identified in 104 BHR+ patients (61.17%), and 132 BHR- patients (25.29%) (P<.001). The areas under the curve (AUCs) of variables used singly for a BHR diagnosis were lower than 0.77. Using joint models of FEF50%, FEF75%, or FEF25%-75% with FENO increased the AUCs to 0.845, 0.824, and 0.844, respectively, significantly higher than univariate AUCs (P <.001 for all). Patients who reported chest tightness (n=75) had lower FEFs than patients who did not (P<.001 for all). In subjects with chest tightness, the combination of FEF50% or FEF25%-75% with EOS also increased the AUCs substantially, to 0.815 and 0.816, respectively (P <.001 for all versus the univariate AUCs). Conclusion: FENO combined with FEF50% and FEF25%-75% predict BHR in patients with normal FEV1. FEF25%-75%. FEF50%, or FEF25%-75% together with EOS also can potentially suggest asthma in patients with chest tightness.