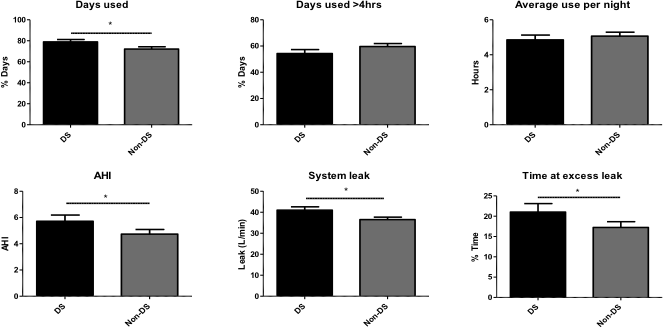
Objective: Children with Down syndrome (DS) have an increased prevalence of obstructive sleep apnoea (OSA). Non-invasive ventilation (NIV) is a common modality of OSA treatment in this cohort. This study aimed to measure adherence and efficiency of NIV delivery in children with DS. Study design: This was a retrospective cohort study involving 106 children with confirmed OSA and home NIV with downloadable data capacity. Children were divided into DS (n=44) and non-DS cohorts (n=62). Adherence, clinical outcomes apnoea-hypopnoea index (AHI), positive airway pressure delivery and leakage were recorded and compared between DS and non-DS cohorts and within the DS cohort based on past surgical history. Results: Significantly greater NIV usage was observed in the DS cohort, they showed more consistent use with an increased percentage of days used relative to their non-DS counterparts (78.95 ± 2.26 versus 72.11 ± 2.14, p=0.031). However, despite greater usage, poorer clinical outcomes in the form of increased AHI (p=0.0493) was observed in the DS cohort, where significantly greater leakage was also shown 41.00 ± 1.61L/min versus 36.52 ± 1.18L/min (p=0.022). Twenty children with DS had prior cardiac surgery; compliance across all parameters was significantly reduced relative to those without. Conclusions: These data confirm that satisfactory NIV adherence is achievable in children with DS. However, we have identified excessive system leak at the machine-patient interface as a factor, which could undermine NIV efficacy in children with DS.